Article Text

Abstract
AIM To investigate breathing rhythm and brain stem autonomic control in patients with Rett disorder.
SETTING Two university teaching hospitals in the United Kingdom and the Rett Centre, Sweden.
PATIENTS 56 female patients with Rett disorder, aged 2–35 years; 11 controls aged 5–28 years.
DESIGN One hour recordings of breathing movement, blood pressure, ECG R-R interval, heart rate, transcutaneous blood gases, cardiac vagal tone, and cardiac sensitivity to baroreflex measured on-line with synchronous EEG and video. Breathing rhythms were analysed in 47 cases.
RESULTS Respiratory rhythm was normal during sleep and abnormal in the waking state. Forced and apneustic breathing were prominent among 5–10 year olds, and Valsalva breathing in the over 18 year olds, who were also most likely to breathe normally. Inadequate breathing peaked among 10–18 year olds. Inadequate and exaggerated breathing was associated with vacant spells. Resting cardiac vagal tone and cardiac sensitivity to baroreflex were reduced.
CONCLUSIONS Labile respiratory rhythms and poor integrative inhibition in Rett disorder suggest brain immaturity. Linking this to an early monoaminergic defect suggests possible targets for the MECP2 gene in clinical intervention. Exaggerated and inadequate autonomic responses may contribute to sudden death.
- Rett disorder
- autonomic system
- brain stem
- dysautonomia
Statistics from Altmetric.com
Rett disorder, causing profound intellectual and physical disability, is caused by MECP2 mutations.1 ,2 Of 56 classic British cases tested, 47 (87%) are mutation positive. There is a wide range of clinical severity.3 ,4 The prevalence of the disorder in the United Kingdom exceeds 1 in 10 000 of the female population.5
Autonomic manifestations include agitation, flushing, pupillary dilatation, and cold extremities relieved by sympathectomy.6 Disrupted sleep staging suggests an early monoamine defect.7 Immaturity is suggested by an infantile distribution of the forebrain circulation8 ,9 and raised serotonin receptor binding in brain stem nuclei.10Irregular breathing in the waking state is associated with non-epileptic vacant spells.11 Low resting cardiac vagal tone and weak vagal response to hyperventilation and breath holding suggest inadequate parasympathetic control.12
Our aim in this study was to characterise the abnormalities of respiratory rhythm and investigate the central autonomic competence in Rett disorder.
Methods
SUBJECTS
Fifty six subjects were referred for diagnostic assessment. Control values came from 11 female volunteers and from previous studies.12-14 Parents received written explanations of procedures and results and provided consent. The ethics committee at South Glasgow University Hospitals NHS Trust approved the study. Rett subjects had all the classic criteria,15 except as follows: no decline in occipitofrontal circumference (n = 6); stagnation in development without regression (n = 4); and seizures before regression (n = 4).
PROCEDURES AND ANALYSES
The subjects sat comfortably with carers while information was obtained by clinical examination and from case records, health questionnaires, and one hour continuous, synchronous, non-invasive autonomic and respiratory monitoring, time locked with video and EEG.
A stretch sensitive resistance plethysmograph at xiphisternal level recorded the amplitude of thoracic and abdominal breathing movements in arbitrary units. A TCM3 monitor (Radiometer, Copenhagen, Denmark) recorded partial pressures of oxygen (Po 2) and carbon dioxide (Pco 2) transcutaneously. A finger photoplethysmograph (Finapres™, Ohmeda, USA) recorded digital arterial blood pressure in waveforms for calculation of beat by beat systolic, mean, and diastolic blood pressure. The central autonomic (brain stem) control of cardioinhibitory activity was monitored by the NeuroScope™ (MediFit Diagnostics, London, UK), which calculates cardiac vagal tone from ECG R-R intervals.16 The cardiac vagal tone is expressed in arbitrary units on a linear vagal scale.17
Breathing movements, levels of blood gases, and blood pressure waveforms were transmitted through an interface—the MedullaLab (MediFit Diagnostics)—and joined the NeuroScope data in a common microcomputer. The VaguSoft software (MediFit Diagnostics) simultaneously recorded ECG, heart rate, cardiac vagal tone, systolic, mean, and diastolic blood pressure, blood gases, and cardiac sensitivity to the spontaneous arterial baroreflex. The EEG was recorded on a 16 channel PL-EEG in the United Kingdom (Walter Graphtek UK, West Sussex, UK) and on an eight channel paper machine (Nihon Ohden, Tokyo Japan) in Sweden. Breath by breath analyses of 47 cases excluded all interruptions.
Baseline functions are defined as autonomic activity during normal breathing with normal levels of blood gases. Control subjects voluntarily hyperventilated and held their breath in accordance with our demonstrations.
STATISTICS
Values are given as mean (SEM). Statistical differences were assessed using analysis of variance (ANOVA) with a two sided Studentt test for probability (p) values, using Minitab for Windows 11.21.
Results
BREATHING RHYTHMS
As previously observed,12-14 no control subject showed spontaneous breathing dysrhythmias. All Rett subjects had some normal rhythm while awake but also showed 5–11 (mean 8) types of abnormal rhythm (figs 1 to 6). Valsalva breathing occurred in 26 of the 47 subjects tested (59%), Biot's breathing in two, and Cheyne-Stokes respiration in 12 subjects with inadequate breathing.

Normal breathing. Ramp inspiration terminated immediately by double phased expiration. Rate below 35 breaths/min, depth average for the individual. Amplitude measured in arbitrary units.

Less frequent breathing rhythms. Top: Cheyne–Stokes breathing—periodic breathing interrupted by central apnoea during which the breathing movements increases gradually in amplitude and decay again into apnoea. Bottom: Biot's breathing—abrupt apnoea followed by equally abrupt regular breathing in which both the apnoea and the regular breathing have variable durations. Amplitude measured in arbitrary units.
Breathing patterns changed with age (fig 7 and table 1). Most forceful and apneustic breathers were under 5 years old and most normal and Valsalva type breathers were older. Combined percentages of breathing dysrhythmias in the 0–9 year age groups (table 1) were higher than in the older age groups (p < 0.005). The percentage of Valsalva breathing in the over 19 year age group was higher than in the youngest group (p < 0.01) or in the 6–9 year old group (p < 0.05). Inadequate breathing was most common under 18 years of age, where Cheyne-Stokes breathing was also seen. Repeat examination of six Rett subjects studied in 198713 indicated the same pattern of change with age.
style in the 10–18 year group. Although there is individual variation and the age group differences do not reach statistical significance, except in a few instances (see text), these trends have been well maintained throughout the 56 recordings made. Values are means; error bars = SEM.

Charts showing the percentages of monitored awake time spent in each type of respiratory rhythm for each age group (see figs 1to 6 for definitions of breathing rhythms): (A) normal breathing; (b) apneustic breathing; (c) forced breathing; (d) inadequate breathing; (e) Valsalva breathing. The forced and apneustic breathing styles are more prominent in the younger age groups, the Valsalva breathing style in the older group, and the inadequate breathing style
Respiratory and autonomic results according to age group
VENTILATORY EFFICIENCY IN RETT DISORDER
Blood gases were recorded transcutaneously in 27 subjects. Carbon dioxide fell during intense hyperventilation and rose during inadequate breathing as oxygen levels fell. Mean lowest and highest Pco 2 values were 4.12 and 5.43 kPa (31 and 41 mm Hg), respectively; in two of 27 feeble breathers (7%) Pco 2 exceeded 7.98 kPa (60 mm Hg). Repeated central apnoea or Valsalva breathing was always associated with a Po 2 below 10.64 kPa (80 mm Hg). Valsalva breathers did not have raised Pco 2, while oxygen fell below 6.65 kPa (50 mm Hg) in 14 of 27 Rett subjects (52%).
BASELINE AUTONOMIC FUNCTION
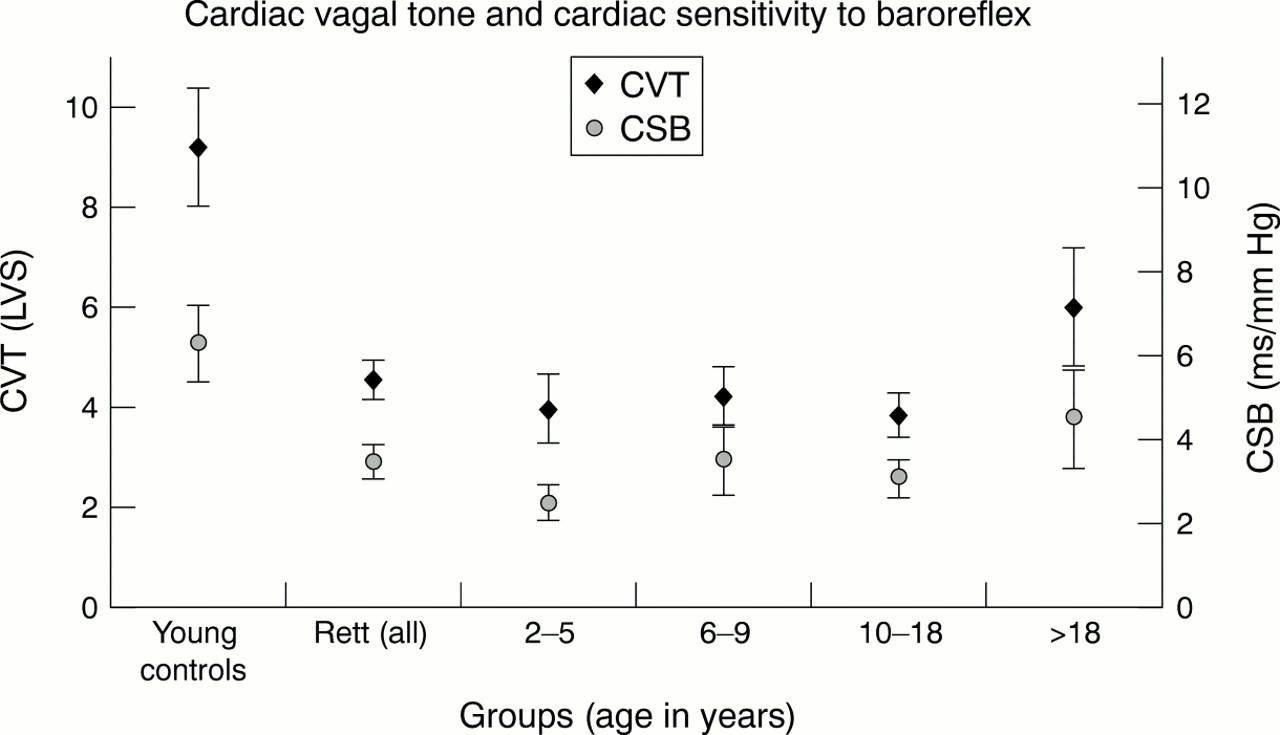
Baseline brain stem autonomic function was analysed in 48 girls aged 2 to 35 years, mean 13.2 years, and in 11 controls aged 5 to 28, mean 10.2 (fig 8). There was no significant difference in mean resting heart rate (mean (SEM): Rett 101 (3.6) beats/min; control 92 (2.5) beats/min) or mean arterial blood pressure (Rett 79 (5.3) mm Hg; control 86 (7.1) mm Hg). Mean cardiac sensitivity to baroreflex was lower in Rett cases than in controls (Rett 3.4 (0.4) ms/mm Hg; control 6.2 (0.9) ms/mm Hg; p < 0.01). Mean cardiac vagal tone was also low in Rett cases: Rett 4.5 (0.4) units; controls 9.2 (1.2) units in the linear vagal scale; p < 0.002).

Autonomic measurements in Rett subjects and controls. The Rett subjects are also divided into age groups. Compared with controls, the mean cardiac vagal tone in the combined Rett group was reduced (p < 0.002), as it was in the various age groups with the exception of the over 18 group. The cardiac sensitivity to baroreflex was also reduced (p < 0.01) in the combined Rett group and in the age groups with the exception of the over 18 group. Values are means; error bars = SEM. CSB, resting sensitivity to baroreflex; CVT, resting cardiac vagal tone measured in the linear vagal scale; LVS, linear vagal scale.
VACANT SPELLS AND ASSOCIATED EVENTS
Epileptiform EEG features increased in sleep and diminished on alerting. Monorhythmic theta waves increased with age. Epileptiform discharges were rarely associated with clinical seizures or vacant spells. Valsalva breathing was sometimes accompanied by 4–5 Hz theta wave activity, and prolonged apnoeas caused EEG flattening. Many vacant spells in 48 of 56 subjects were associated with involuntary movements and dystonic postures and appeared during shallow breathing, long breath holds, central apnoeas, apneusis, and Valsalva breathing.
EFFECTS OF BREATHING DYSRHYTHMIAS ON AUTONOMIC FUNCTION
Voluntary hyperventilation was accompanied by increased mean blood pressure, promptly countered by increased cardiac vagal tone with a consequent decrease in heart rate to control the blood pressure, after which heart rate was restored to normal (fig 9). Vagal tone remained increased during hyperventilation and was withdrawn when hyperventilation ceased. During spontaneous hyperventilation in Rett subjects (fig 9), cardiac vagal tone increased transiently but was withdrawn and reinstated only after the hyperventilation ended. The increase in the mean blood pressure started by the onset of hyperventilation was thus uncontrolled.
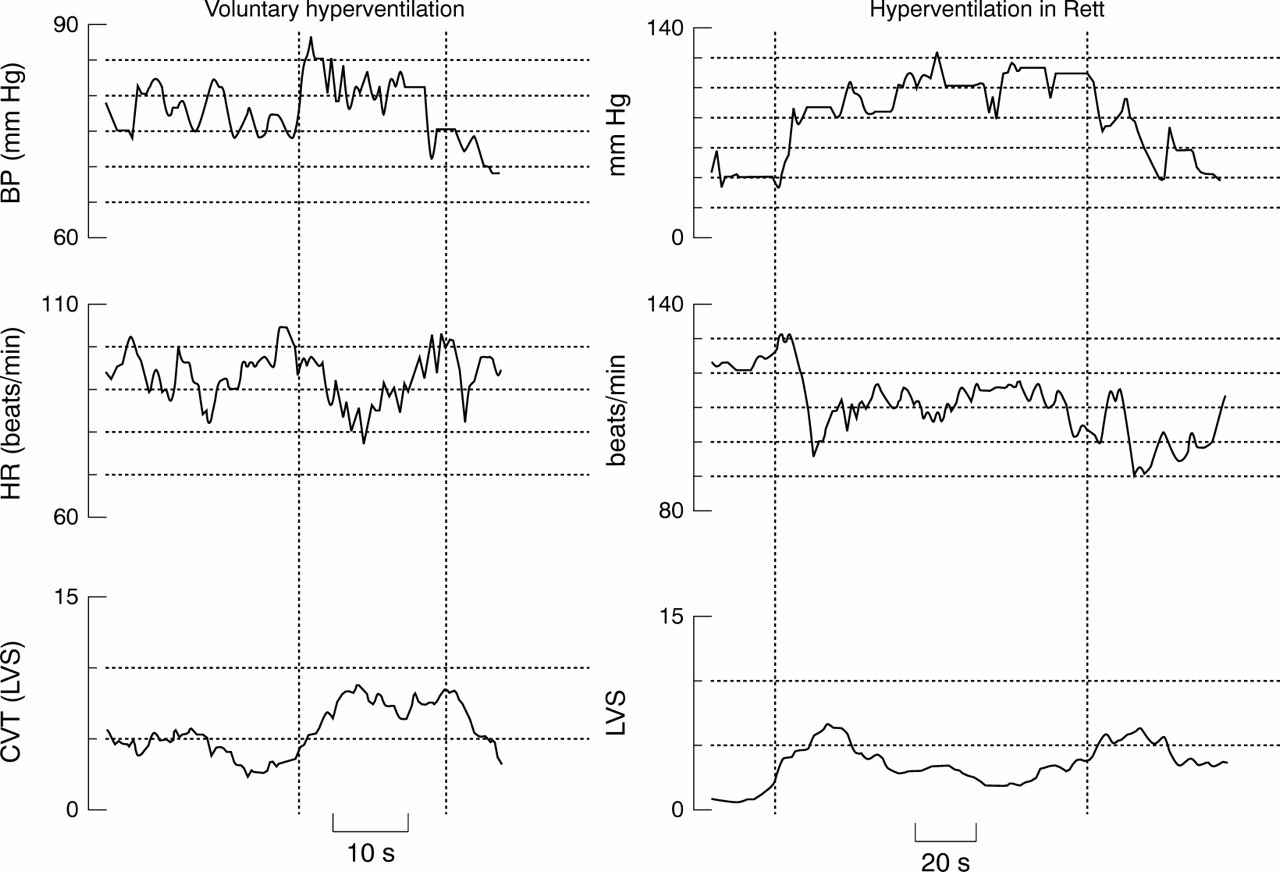
Effects of hyperventilation on sympathovagal balance: control (left) and Rett case (right). The periods of hyperventilation are enclosed with broken vertical lines. Note the sustained increase in cardiac vagal tone in the normal girl, in contrast to vagal withdrawal in a Rett case. Note also the contracted time scale in the Rett diagram. BP, mean arterial blood pressure representing sympathetic activity; CVT, cardiac vagal tone (measured in linear vagal scale (LVS)); HR, heart rate.
Both cardiac vagal tone and cardiac sensitivity to baroreflex reflecting parasympathetic control were withdrawn at the beginning of the voluntary breath hold in control subjects and restored immediately at the end. The cardiovascular system was therefore under the sole influence of the sympathetic system at that time (fig 10).

Effects of breath holding on sympathovagal balance and baroreflex function in a Rett case and a control. The periods of breath holds are enclosed by broken vertical lines. Note the normal smooth withdrawal of cardiac vagal tone and which leaves the cardiovascular control to the sympathetic system.In the Rett case, this manoeuvre unmasked the inadequate restraint of the sympathetic system, indicated by oscillation of blood pressure and exaggerated changes in heart rate. BP, mean arterial blood pressure representing sympathetic activity; CVT, cardiac vagal tone (measured in linear vagal scale (LVS)); HR, heart rate.
In the Rett cases, breath holding caused prompt withdrawal of cardiac vagal tone and cardiac sensitivity to baroreflex, as in the controls, but the increase in sympathetic activity at the beginning of breath holding caused “ringing” (oscillation) of blood pressure, indicating the poor negative feedback regulation (fig 10).
RISK FACTORS IDENTIFIED IN RETT DISORDER
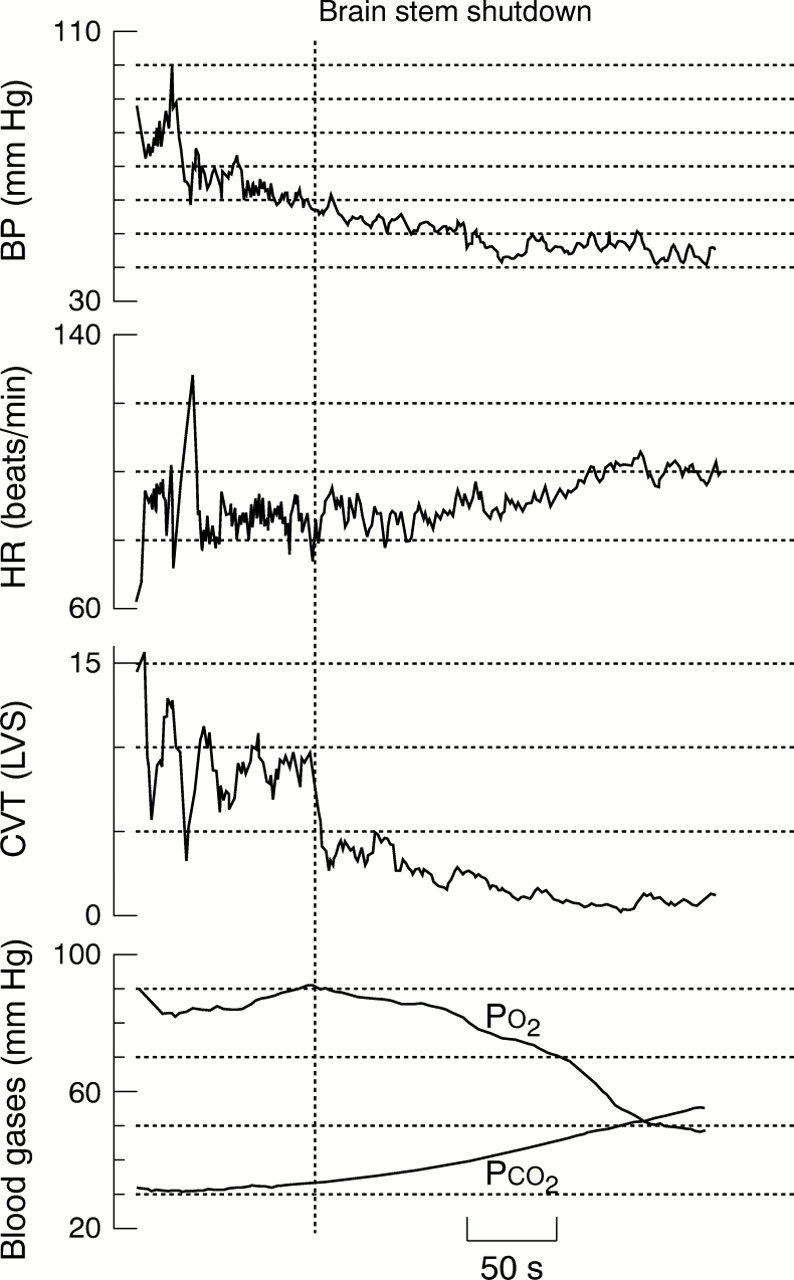
Five Rett subjects developed a progressive decrease in blood pressure with diminishing cardiac vagal tone and cardiac sensitivity to baroreflex. Mean arterial blood pressure approached 40 mm Hg, the level associated with spinal transection; cardiac sensitivity to baroreflex and cardiac vagal tone came close to zero, and heart rate approached the intrinsic rate of the sinoatrial node, suggesting lower brain stem shutdown (fig 11). The EEG showed very low voltage or flat recordings, and transcutaneous oxygen levels fell. These episodes followed repeated or prolonged periods of Valsalva manoeuvres, hyperventilation, or poor ventilation. The longest such shutdown lasted three minutes.

Brain stem shut down in a girl of 11 years. The vertical broken line marks the beginning of the autonomic shutdown (see text). BP, mean arterial blood pressure representing sympathetic activity; CVT, cardiac vagal tone (measured in linear vagal scale (LVS)); HR, heart rate; Po 2 and Pco 2, transcutaneous partial pressure of oxygen and carbon dioxide.
A background of feeble breathing with low Po 2and raised Pco 2 can lead to repeated episodes of exaggerated simultaneous increases in cardiac sensitivity to baroreflex, cardiac vagal tone, and blood pressure (fig 12). The term “brain stem storm” is appropriate for this event, as the functional indices of the whole brain stem—rostral, caudal, and dorsal—were simultaneously and momentarily increased. Such sudden large increases in vagal tone with poor ventilation, raised carbon dioxide, and hypoxia carry a risk of cardiac arrest.
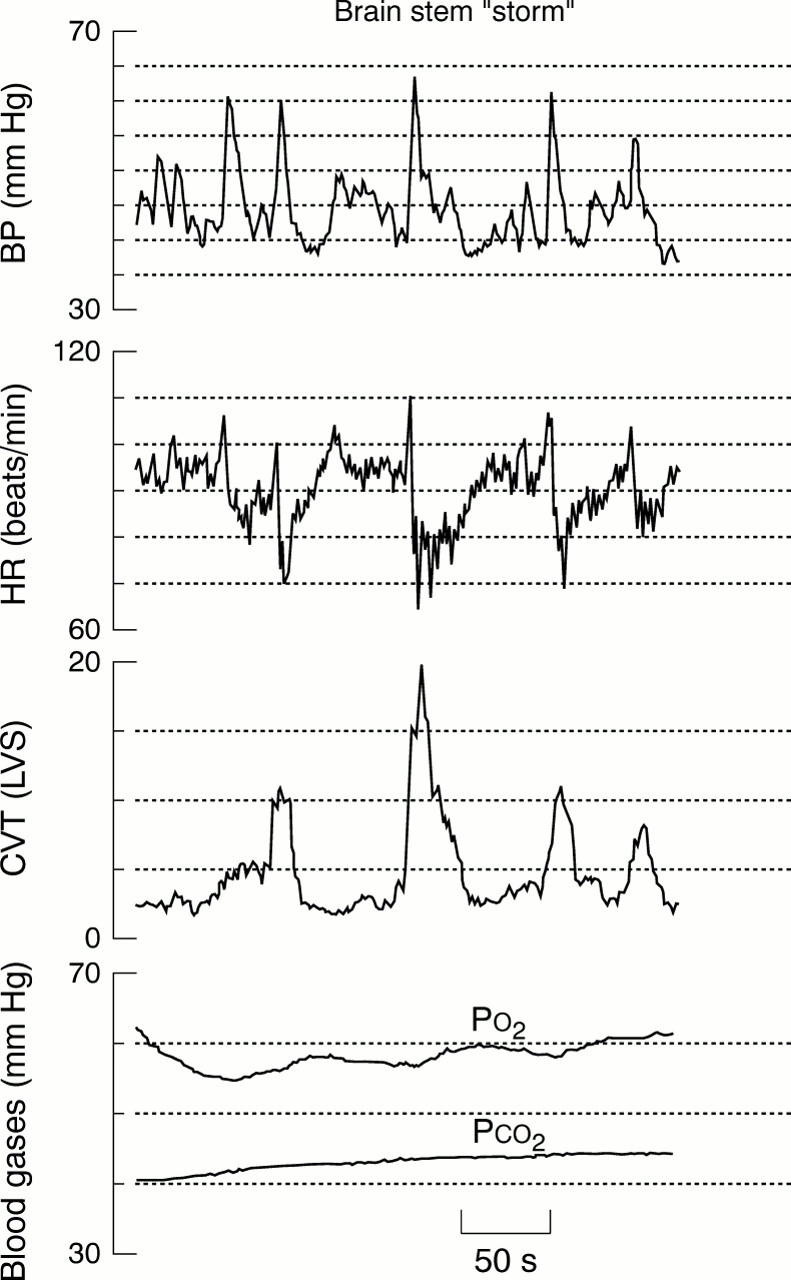
“Brain stem storm” in a girl of 11 years, illustrating spontaneous and exaggerated excitation of the brain stem during feeble breathing. Oxygen level oscillated below 60 mm Hg and at every trough there were spikes in blood pressure and heart rate. On four occasions there were spikes of cardiac vagal tone causing sharp and transient bradycardia. The exaggerated simultaneous spikes of blood pressure, heart rate, and cardiac vagal tone constitute a brain stem storm (see text). BP, mean arterial blood pressure representing sympathetic activity; CVT, cardiac vagal tone (measured in linear vagal scale (LVS)); HR, heart rate; Po 2 and Pco 2, transcutaneous partial pressure of oxygen and carbon dioxide.
We observed episodes of brain stem activity which did not conform to the expected physiological activation of the neurones involved. Normally, output from autonomic neurones is continuously adjusted through reflexes or pacemaker neurones according to body needs. The term “brain stem epilepsy” seems appropriate for the brief, widespread, aberrant activation of the brain stem neurones (fig 13), although no epileptiform activity was recorded at the cortex. This differed from brain stem storm in that the known physiological predisposition to increased brain stem excitability—such as feeble breathing, low Po 2, and high Pco 2—observed in brain stem storm were not present. Epileptic involvement of the respiratory neurones may be an additional hazard in Rett disorder.

“Brain stem epilepsy” in a girl of 13 years. The breathing rhythm was normal and transcutaneous gases were within normal limits. The exaggerated and repeated simultaneous sharp increases in blood pressure, heart rate, and cardiac vagal tone—best seen at the beginning and end of the traces—represent widespread aberrant excitation of the brain stem (see text). BP, mean arterial blood pressure representing sympathetic activity; CVT, cardiac vagal tone (measured in linear vagal scale (LVS)); HR, heart rate; Po 2 and Pco 2, transcutaneous partial pressure of oxygen and carbon dioxide.
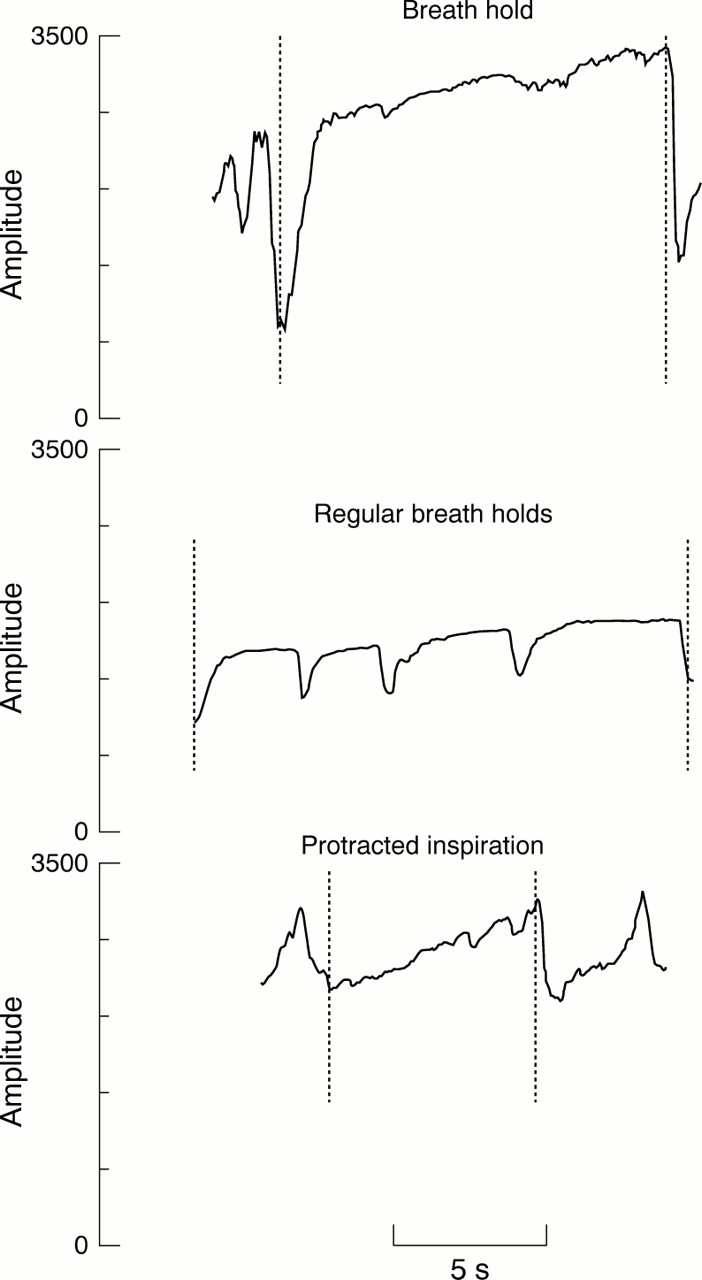
Apneustic breathing style. Top: breath hold—a single fast full inspiration followed by a delayed fast expiration. Middle: regular breath holds—episodes of breath holding. Bottom: protracted inspiration—a prolonged and continuous inspiration ended abruptly by full expiration (achieved fast, often forcefully), insufficient to obstruct venous return. Amplitude measured in arbitrary units.
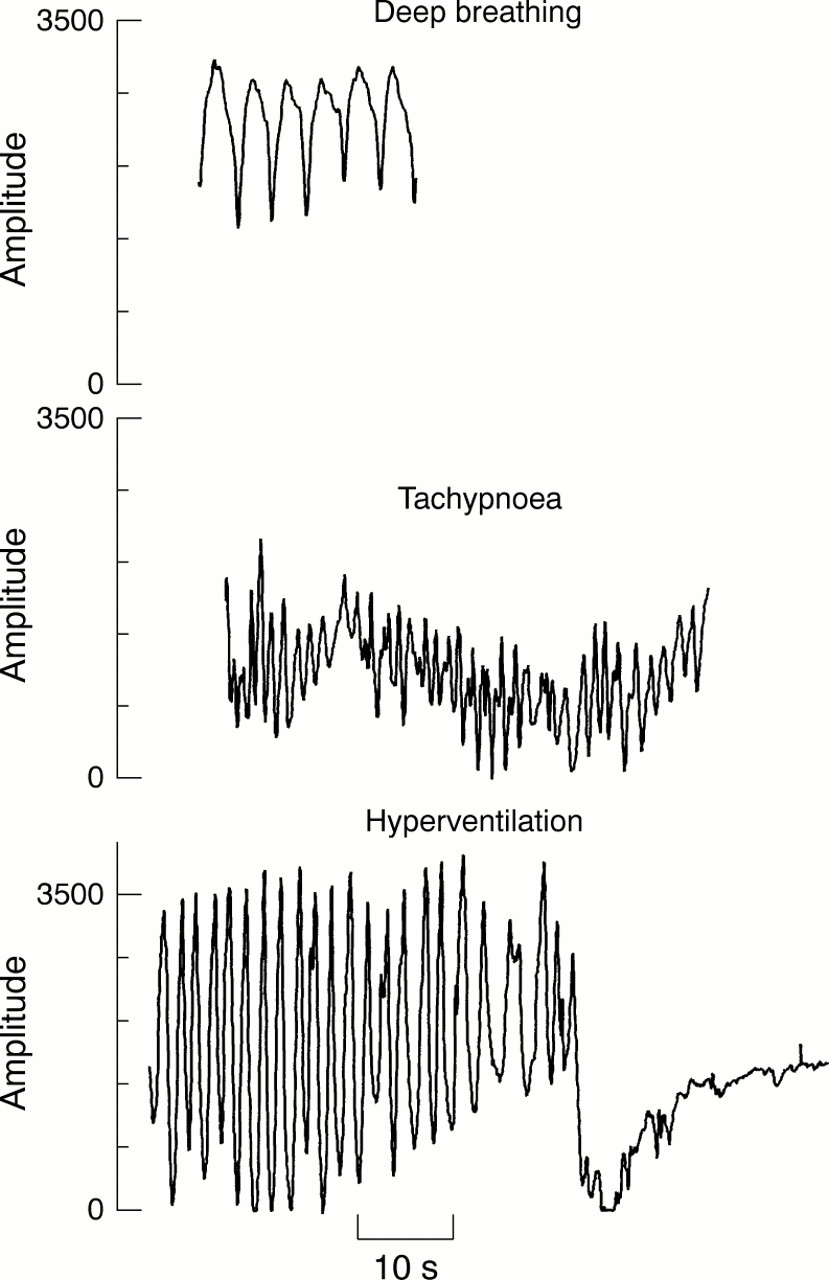
Forceful breathing style. Top: deep breathing—episode of exaggerated inspirations followed immediately by exaggerated expirations without causing central apnoea; rate below 35 breaths/min, depth must be well above average for that person. Middle: tachypnoea—episode of rapid inspirations followed immediately by expirations without causing central apnoea. Rate 35–45 breath per minute, depth average or greater for that person. Bottom: hyperventilation—episode of exaggerated inspirations followed immediately by equally exaggerated expirations contributing directly to a central apnoea. Amplitude measured in arbitrary units.

Inadequate breathing style. Top: rapid shallow breathing—episode of shallow inspiration followed immediately by equally shallow expiration; rate above 35 breaths/min, depth below average for that person. Middle: shallow breathing—episode of shallow inspiration followed immediately by equally shallow expiration; rate below 35 breaths/min, depth must be below average for that person. Bottom: central apnoea—cessation of breathing movement at the end of expiration. Amplitude measured in arbitrary units.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
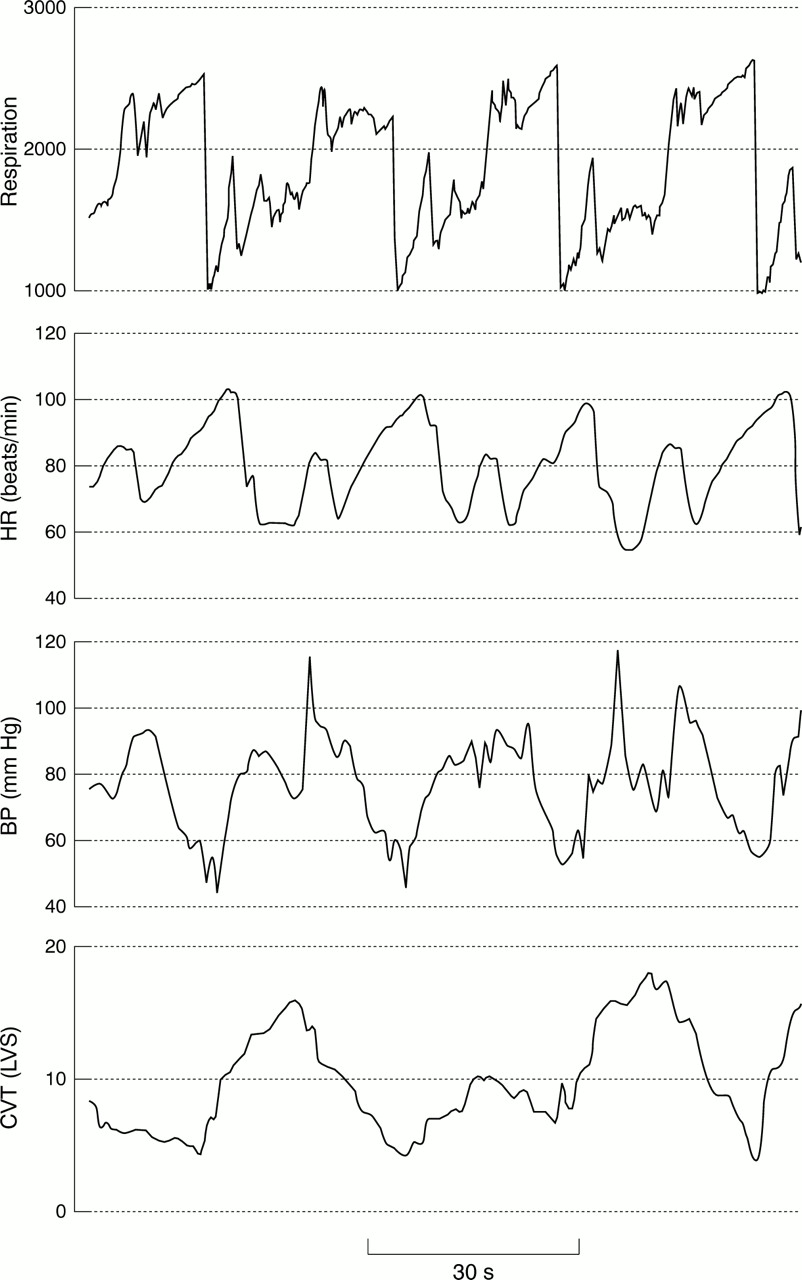
Valsalva breathing style. Valsalva manoeuvre: breath holds or protracted inspiration capable of raising intrathoracic pressure sufficiently in magnitude and duration to reduce venous return and cause characteristic blood pressure (BP) or heart rate (HR) changes (saw toothed responses with rebounds). CVT, cardiac vagal tone; LVS, linear vagal scale. Amplitude measured in arbitrary units.
Discussion
PHYSIOLOGICAL BASIS OF THE AUTONOMIC MEASUREMENTS
The principles underlying neuronal control of cardiorespiratory function are well documented and our methods are discussed fully in earlier reports.12 ,18 However, we offer a brief physiological explanation here, with comments on our results.
Sympathetic activity is closely related to mean arterial blood pressure19 and can thus be monitored indirectly by measuring blood pressure. In humans, the brain stem controls blood pressure directly through the common vasomotor pathway in the spinal cord.20 Bilateral transection of the common vasomotor pathway abolishes blood pressure control, and the mean arterial blood pressure collapses to 40 mm Hg. Normal mean baseline arterial blood pressure in Rett disorder indicates normal sympathetic function in the brain stem.
Excitation of the baroreceptor, combined with the rise in arterial pressure caused by ejection of blood from the left ventricle, inhibits the sinoatrial node,21 delaying the onset of the following cardiac cycle, as reflected in the R-R interval. As blood is ejected into the arteries at every cardiac cycle, thus stimulating the baroreceptors,22 there are rapid and quantifiable pulse synchronised changes in R-R intervals. These are measured continuously by the NeuroScope™.16 Baroreceptor signals are the main source of excitation for the cardiovagal motor neurones in the medulla.23 The cardiac vagal tone is the end result of impulses carried in the vagus nerve and regulated through integrative processes in the nucleus of the tractus solitarius, nucleus ambiguus, and the bulbar reticular formation.24 Being the only inhibitory output of the cardiorespiratory integrative system, cardiac vagal tone is very important in rapid cardiovascular responses and is a major contributor to integrative inhibition in the system. The normal mean value for cardiac vagal tone in young supine adults breathing quietly is 10 arbitrary units in the linear vagal scale, falling to zero at full atropinisation.17 The cardiac vagal tone is a more direct indicator of central cardiovascular parasympathetic output than the surrogate index respiratory sinus arrhythmia. The cardiac sensitivity to baroreflex is the increase in pulse intervals per unit change in systolic blood pressure. It is calculated by quantifying cardiac responses to ejection pressures in each cardiac cycle as ΔRR/ΔSBP, where ΔRR is the difference between present and previous ECG R-R intervals and ΔSBP is the difference between the systolic blood pressure values in two preceding cardiac cycles.26 The cardiac sensitivity to baroreflex indicates the overall gain in the negative feedback in the baroreflex system set up in the nucleus tractus solitarius. Consistently low baseline cardiac vagal tone and cardiac sensitivity to baroreflex in Rett cases indicates reduced integrative inhibitions in both the nucleus tractus solitarius and the nucleus ambiguus.
During the normal initiation of an end of inspiration breath hold, the lungs fill with air and stimulate the slow-adapting pulmonary stretch receptors, leading to reduction in cardiac vagal tone and cardiac sensitivity to baroreflex. This explains the withdrawal of cardiac vagal tone and cardiac sensitivity to baroreflex at the onset of the normal breath hold. The central inspiratory drive at the beginning of the breath hold increases sympathetic tone and further decreases cardiac vagal tone and cardiac sensitivity to baroreflex. As long as the lungs are inflated, the sympathetic system remains in full control of the cardiovascular system, with minimal parasympathetic activity. Our results show that healthy people can cope with the reduced negative feedback in the parasympathetic system during a breath hold, whereas this manoeuvre is precarious in Rett disorder.
BRAIN STEM FEATURES OF RETT DISORDER
We have shown that the baseline brain stem functions (breathing rhythm, cardiac sensitivity to baroreflex, and cardiac vagal tone, which are maintained by complex integrative inhibitions) are affected in the Rett disorder, while baseline sympathetic tone, maintained by pacemaker activity, is preserved. Moreover, sympathetic responses during hyperventilation are poorly regulated in Rett disorder, indicating insufficient reciprocal innervation and lack of integrative inhibition within the cardiorespiratory neurones. The oscillation of blood pressure during breath holding in Rett disorder indicates lack of parasympathetic restraint of the sympathetic system because the cardiovascular system is restrained through a parasympathetic negative feedback system.27 That Rett subjects did maintain normal breathing while asleep may reflect improved inhibitory integration in the brain stem during sleep. The breathing dysrhythmias while awake may suggest poor integration at higher centres like the hypothalamus and the limbic cortex, where “wakefulness drive” of breathing is significantly modulated.28
The apneusis (protracted inspiration) commonly seen in the youngest Rett girls suggests a serotonin (5-HT) defect in the brain stem, as the termination of inspiration to allow initiation of expiration in humans depends in part on 5-HT1A receptors.29 Valsalva breathing was seen in older Rett survivors, the severely affected having died in adolescence. Valsalva breathing can achieve adequate CO2expulsion against inappropriate contraction of the glottis, but also contributes to aerophagy.11 Inadequate ventilation is often overlooked but it indicates weak central respiratory drive with reduced inhibition of cardiac vagal tone, rise in Pco 2, and fall in Po 2. The combination of hypercapnia and hypoxia optimally stimulates the peripheral chemoreceptors and, combined with weak central respiratory drive, leads to maximal cardiovagal excitation such as was seen in brain stem storm (fig 12). Brain stem shutdown may be due to postactivation or postictal neuronal quiescence after severe brain stem activation caused by forceful breathing (fig 11). Brain stem epilepsy (fig 13) is not unique to Rett cases, and we have observed it during routine autonomic examination in elderly people with syncope and in other patients with epilepsy.
POTENTIAL CLINICAL INTERVENTIONS IN RETT DISORDER
On the basis of our results, the brain stem neurotransmitters may offer a means of clinical intervention. L-glutamate is required for baroreceptor input.24 Serotonin receptor type 5-HT4, angiotensin-II, and enkephalin are all modulators of cardiac sensitivity to baroreflex at the nucleus tractus solitarius.30 ,31 γ-Aminobutyric acid (GABA) is used to modulate cardiac sensitivity to baroreflex and cardiac vagal tone by supramedullary centres and vagal afferents from the lungs.24 The muscarinic cholinergic system modulates cardiac vagal tone and baroreflexes.25 ,32 Second messengers such as cAMP and diacyl glycerols, necessary for nerve signal transduction, may become depleted in brain stem neurones, leading to central apnoea (Harkness RA, personal communication, and33 ,34). Clinical manipulation of these factors by either supplementation or pharmacological means may be beneficial in Rett disorder.
CONCLUSIONS
Compelling clinical, neurophysiological, and neuropathological evidence points to a prenatal brain defect with early brain stem involvement in Rett disorder.10 ,35 ,36 The labile breathing rhythms, the reduction in baseline cardiac vagal tone and cardiac sensitivity to baroreflex comparable to that of neonates,37 and signs of the inability to restrain sympathetic responses in Rett disorder indicate brain stem immaturity and a lack of integrative inhibition, with consequent failure to respond normally to physiological demands. This explains many vacant spells and some sudden deaths.38 ,39 Rett disorder is a congenital dysautonomia. The slow development, regression, and limited growth seen in Rett disorder closely match the concepts of the MECP2 gene failing to regulate target genes involved in development, thereby initiating a cascade of problems. Genes controlling brain stem neurotransmitters offer potential for clinical interventions and insight into this disorder. Our methods have proved helpful in studying the Rett disorder and will assist in the diagnosis of other conditions and in monitoring clinical interventions.
Acknowledgments
We acknowledge support and collaboration from the families, the young volunteers, Rett Syndrome Associations UK, National, Swedish, and International, Swedish Rett Centre and Lyan staff, Pavel Belichenko, Dawna Armstrong, Bengt Engerstrom. Southern General, Bollnäs, Sundsvall, and Östersund Hospitals supplied additional equipment. Swedish grants were from Irma och Arvid Larsson-Röst's Memorial Foundation, Anna Brita och Bo Castegren's Memorial Foundation, Östersund Hospital Foundation for Medical Research, and Marcus och Amalia Wallenbergs Memorial Foundation.