Article Text

Abstract
OBJECTIVE The surgical treatment of intractable Tourette's syndrome is controversial. Experience with 17 consecutive patients treated between 1970 and 1998 is reviewed and the efficacy and safety of surgical treatment is assessed.
METHODS These patients were retrospectively reclassified into subtypes according to the protocol of the Tourette's Syndrome Study Group. One patient was excluded from the study. Ventriculography based stereotactic zona incerta (ZI) and ventrolateral/ lamella medialis thalamotomy (VL/LM) were performed on all patients. The preoperative, postoperative, and late tic severities were assessed by the tic severity rating scale. The median follow up of 11 patients (65%) was 7 years (range 3.5–17 years) and six patients were lost to long term follow up.
RESULTS Median age was 23 years (range 11–40) at the time of surgery. Median duration of illness was 14 years (range 3–33). The mean preoperative motor and vocal tic severities were estimated to be 4.44 (SD 0.63) and 3.81 (SD 0.66), respectively. Unilateral ZI lesioning and VL/LM lesioning selected by asymmetry of symptoms provide an effective control of tic severity (p motor and vocal<0.001). In attenuation of contralateral symptoms, a second surgical intervention in the relevant side could reduce tic severity sufficiently (p motor<0.01; p vocal<0.005). Transient complications occurred in 68% of patients. Only one permanent complication was registered in six patients followed up after unilateral surgery. Two out of five patients followed up after bilateral surgery had disabling side effects of surgery.
CONCLUSIONS ZI and VL/LM lesioning provide a significant long term reduction of tic severity in intractable Tourette's syndrome. Adequate selection of the side of first intervention might prevent the patient from increased risk of bilateral surgery.
- Gilles de la Tourette's syndrome
- infrathalamic and thalamic lesioning
Statistics from Altmetric.com
The interpretation of Gilles de la Tourette's syndrome has changed radically since the first description of the disease in 1885.1-3 Recent studies suggest that Tourette's syndrome and chronic tic disorders seem to follow an autosomal dominant pattern of inheritance, with varying degrees of penetrance. Its expression is influenced by sex, with male preponderance.4-6Tourette's syndrome is the most complex manifestation of a group of related tic disorders. The character of the tics is similar throughout the range, and it is one of the fastest growing diagnoses with a prevalence of from 2.9 to 5.2/10 000 population.7 8 Tic disorders usually develop in childhood and they will remit completely in 30%-40% of patients by late adolescence with an additional further improvement of 30% in later years.9 Drug therapy, driven by the most functionally disabling symptoms, consists of various therapeutic agents including haloperidol and pimozide.10Despite the best psychopharmacological and behavioural therapeutic efforts, a few patients have residual debilitating symptoms, including self injurious behaviour. The management of this malignant manifestation of Tourette's syndrome remains controversial and a minority of patients are finally referred for surgery.11-14
Surgical results with intractable Tourette's syndrome are mostly anecdotal, without any firm statistical conclusions.15 We summarise our experience with 17 consecutive patients with intractable Tourette's syndrome treated by infrathalamic and/or thalamic lesioning. Our primary aim was to assess the feasibility and safety of this method by retrospective evaluation of the clinical and follow up data. In addition, we describe the potential characteristics of malignant Tourette's syndrome. Target selection and the validity of zona incerta (ZI) lesioning are discussed.
Patients and methods
Seventeen patients with medically intractable Tourette's syndrome were treated at the Stereotactic and Functional Neurosurgery Department of Freiburg (Germany) between 1970 and 1998. Their records were retrieved from the Freiburg stereotactic functional neurosurgery database (FSFND) and were reclassified according to the protocol of the Tourette's Syndrome Study Group.16 Only those patients who fulfilled the minimal criteria for Tourette's syndrome were included in the study.
We applied a simple five point scoring system (tic severity rating scale, TSRS) to quantify preoperative and postoperative tic severity.17 The rating process was based on the complexity and frequency of motor and vocal tic phenomena. The assessment was carried out independently by two of us (TBB, PCW) not involved in the surgery. The different values from the rates were then combined and averaged. We compared preoperative, immediate, and late outcome TSRS scores by paired t test. The same process was applied to preoperative and to late outcome scores in unilateral and bilateral surgical groups. A p value<0.05 was considered to be significant.
Five out of 16 patients (31%) were lost for late outcome assessment. The median follow up of the remaining 11 patients was 7 years (range 3.5–17 years). The follow up period took place between 1990 and 1999. The neurological status, tic severity, and treatment satisfaction index (TSI) were registered in the FSFND.
INDICATION AND OPERATIVE TECHNIQUE
All patients referred to surgery were previously treated by multiple non-surgical methods (multidrug protocols, behavioural therapy, psychoanalysis, hypnosis etc) without any documented long term benefit. The side of the surgery was selected by the asymmetry of clinical manifestations of Tourette's syndrome. Second stage surgery was only indicated when the contralateral symptoms increased to a disabling level after the first intervention.
All patients were operated on under local anaesthesia with light sedation. The target coordinates were computed by ventriculography using the Riechert-Mundinger System (Fischer Co, Germany). The ventral border of the foramen of Monro (FM) and posterior comissure (PC) line was determined.18 ZI was targeted at 12 mm behind the ventral border of FM, 3–5 mm below the FMPC line, and 8–9 mm lateral to the border of the third ventricle. The lamella medialis thalamus (LM) was selected at 7 mm posterior to the FM, 4 mm above the FMPC line and 6.5 mm lateral to the border of the third ventricle. The coordinates of the ventrolateral nuclei (VL) were computed as 10–13 mm behind the FM, between 0 and 1.5 mm from the FMPC line, and 9–10 mm lateral to the border of the third ventricle. Multiple radiofrequency lesions (3–4) up from the target site were performed using a string electrode (1 mm diameter, 5–7 mm exposed tip) and a thermocontrolled straight electrode (2 mm diameter 2 mm exposed tip) (Fischer Co, Germany). The lesioning indices were chosen as 80–90 mA, 25 V, 20–25 seconds. Nine of 16 patients (56%) were operated on bilaterally. ZI lesioning was performed in all but one patient (patient 7). ZI and VL/LM targets were selected in 11 patients (69%).
Results
PATIENT CHARACTERISTICS
The relevant clinical data of patients and time of follow up are shown in table 1. Median age of 16 patients (11 male and five female) at the time of surgery was 23 years (range 11–40). The median onset of the symptoms before surgery was computed as 6 years (range 4–12). The median duration of disease was 14 years (range 3–33 years). Neurological deficits and any abnormality disclosed by ventriculography, EEG, or CT were not registered. Brain MRI in patient 7 showed bilateral calcification of the basal ganglia. All but one patient did not meet the current diagnostic criteria for Tourette's syndrome. Attention deficit hyperactivity disorder and obsessive compulsive disorder were documented in patients 11, 14, and 15.
Summary of clinical data and follow up time1-150
POSTOPERATIVE AND LATE TIC SEVERITY REDUCTION
The immediate tic severity reduction is shown in table 2. The late tic severity reduction in the follow up group of patients is presented in table 3. The significant tic severity reduction was found to be long lasting. Our results did not show any difference between motor and vocal tic severity control. All patients, except two in the follow up group, seemed to be satisfied with treatment. Interestingly, the sensory tic phenomena were also improved in patient 11. Almost all patients remained on multidrug therapy. The late reduction in tic severity in the group of patients operated on bilaterally or unilaterally is shown in tables 4 and 5. The alleviation of vocal tics was more significant than that of motor tics. The reduction in motor tic severity in the bilateral surgical group was less significant than in the unilateral group. Unilateral ZI and VL/LM lesioning selected by asymmetry of symptoms provided an effective control of tic severity. In cases of contralateral symptom attenuation, surgical intervention on the relevant side could sufficiently reduce tic severity.
Immediate results in total group of patients
Late results in follow up group of patients
Late results after bilateral interventions
Late results after unilateral infrathalamic and thalamic lesioning
POSTOPERATIVE AND LATE COMPLICATIONS
There was no operative mortality. Cerebellar signs, dystonia, and dysarthria were detected in 11 of the total group (69%) and in nine of 11 patients in the follow up group (81%). Postoperative morbidity in six of nine patients (66%) proved to be transient (table 6). Three patients in the follow up group (27%) had disabling side effects of surgery. In patient 13, an intraoperative complication of contralateral ZI lesioning resulted in disabling hemiballism. In patient 14, after a very transient improvement from left ZI and VL lesioning, the patient refused the contralateral operation.
Summary of the target sites and complications of bilateral and unilateral interventions
Discussion
The pathology of Tourette's syndrome has not been clearly defined. A decrease in volume of the corpus striatum due to underdevelopment, with additional gliosis in the ventromedial nuclei of the thalamus, has been described.19 20 Brain MRI sometimes shows a significant reduction in left striatal-pallidal volumes, with deviations of lateral ventricular volume and asymmetry in patients with Tourette's syndrome compared with normal controls.21 22 These findings led to speculation on brain lateralisation in the disease and suggested a role for sex hormones as relevant developmental factors.23 In the group that underwent unilateral surgery we were not able to identify any obvious laterality. Four male patients had surgery on the right, but only one of the three patients with left side surgery was male. (table 6). Adequate selection of the side of first intervention might prevent the patient from increased risk of further surgery.24 Basal ganglia MR volumetry and SPECT/PET studies might improve the side selection for surgery.
DIAGNOSIS OF TIC DISORDERS
Tourette's syndrome was initially diagnosed by the clinical manifestations of the illness, resulting in much confusion in clinical practice.3 Tic disorders have recently been redefined by various complex diagnostic criteria and the time course of tic phenomena.16 Tourette's syndrome is commonly accompanied by various behavioural disturbances—for example, obsessive compulsive disorder and attention deficit hyperactivity disorder.9 25 Sensory tics, reported to be a common and distinctive feature of Tourette's syndrome, are defined as the subjectively experienced component of neural dysfunction below the threshold for motor and vocal tic production.26 Sensory tics and overlapping obsessive compulsive disorder phenomena are not consistently delineated. Tics may also accompany various other neurological conditions and are than classified as secondary tic disorders. This condition is usually seen in conjunction with other movement disorders.
There are various possible underlying conditions that may result in the symptoms described as tic disorders. Recent research has implicated group A β haemolytic streptococcusinfection (GABHS) as a possible environmental trigger in families genetically susceptible to various movement disorders, including Tourette's syndrome.27 28 However, these findings might explain only a part of its aetiology. The artificial separation of Tourette's syndrome, involuntary movement disorders, and compulsive phenomena are not consistently supported by clinical evidence.13 29 30 Interestingly, our patients' records did not disclose any direct evidence of hereditary transmission, except for patient 14; mild head jerking by the patient's father was registered. Possible GABHS infection might have played a part in admission to hospital for pneumonia in patients 7 and 10 and tonsillectomy in patient 2 (table 1). In this patient, tics appeared in the year when a severe tonsillitis was finally operated on. The sex distribution in our case series and the time onset of symptoms was in accordance with the literature.9 25 On the other hand the overlapping of obsessive compulsive disorder and attention deficit hyperactivity disorder were documented in only three patients.15
Malignant Tourette's syndrome may represent a special subgroup of the tic range.9 12 14 The controversies about management of this subgroup make a strong case for investigation separately from the less florid manifestation of the syndrome. Typical malignant Tourette's syndrome is characterised as a medically intractable condition with a persistently high score on tic severity rating scales, resulting in self injurious behaviour or severe impairment of social function. Disappearance of waxing and waning phenomena in the dynamics of Tourette's syndrome was documented in all patients. Management of these young patients with malignant Tourette's syndrome ( median age at surgery 23 years) could be very difficult because of the lifelong nature of the illness. The retrospective nature of the study does not allow us to give clear cut selection criteria for surgery. However, based on our findings, we propose to include the permanence of a high score in TSRS with lack of waxing and waning phenomena with a documented medically intractable condition.
OUTCOME ANALYSIS
Tics are probably the most difficult of all movement disorders to rate with validity and reliability.17 31 32 They are remarkably variable in their clinical range and most patients have some temporary volitional control over their movements. Permanent disabling tic symptoms were documented in all our patients. The retrospective approach of the study allowed the use of a simple tic severity assessment. In this context our results indicate that the reduction in tic severity after ZI and VL/LM lesioning remains long lasting. The motor tic reduction seemed to be less predictable but significant. We were not able to detect a best responder subgroup within our patients. In half of our patients contralateral intervention was indicated to alleviate the attenuated contralateral symptoms. The bilateral interventions could provide effective long term tic reduction but there is a higher risk for permanent morbidity. Lesioning of the ZI and VLT is clearly a procedure with higher risk, but more than 50% immediate morbidity is transient.33 34
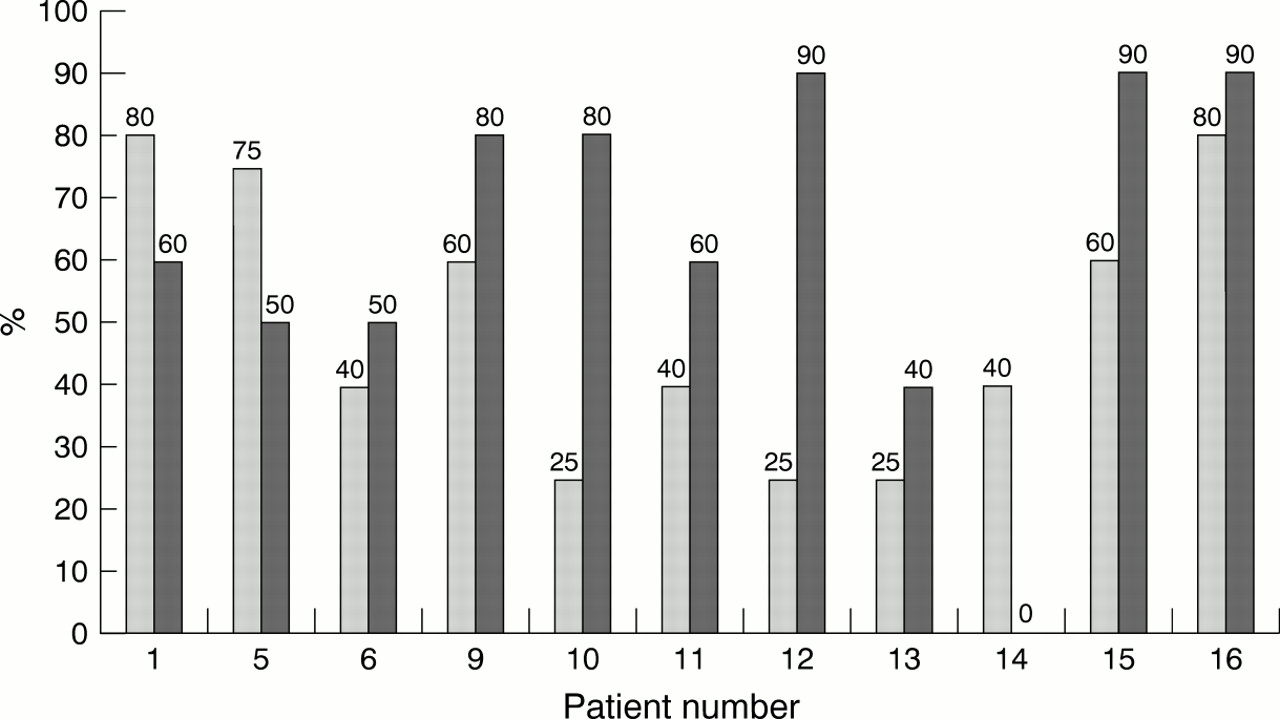
Despite the nowadays unacceptable high morbidity risk almost all patients seemed to be satisfied with their treatment. The further evaluation of follow up data suggest that the fluctuation of symptoms of Tourette's syndrome remained below the disabling level, allowing the patients to function independently after surgical intervention and to respond again to non-surgical treatments. However, our long term results seem to challenge using reduction of symptoms as the only methodology for outcome assessment. Even with very simple dual outcome assessment, we were not able to detect an association between reduction in tic severity and patient satisfaction (figs 1 and 2). Our findings suggest a careful interpretation of long term outcome data that should in the future include the quality of life rating scales.

Comparison of the rate of reduction in vocal tic severity with the treatment satisfaction index (TSI) disclosed controversies of outcome assessment. TSI is a simple visual scale from absent (0) to absolute satisfaction (100%) estimating satisfaction with the result of surgical treatment. Light columns=tic severity reduction rate; dark columns=treatment satisfaction index.

Comparison of the rate of motor tic severity reduction with the treatment satisfaction index (TSI). Further explanation as figure 1.
TARGET SELECTION
The relevant neuroanatomical model for Tourette's syndrome surgery has been intensively reviewed by Rauch et al.15 Only the recent contributions are summarised here. Brain PET studies have provided data suggesting that the striatolimbic-premotor area is uncoupled in Tourette's syndrome compared with control subjects. However, the metabolic rate of the striatal-sensorimotor region was positively correlated with Tourette's syndrome.35 The ventral striatum, corpus callosum, thalamus, and midbrain were reported as potentially important neural substrates of Tourette's syndrome.25 36 37 All structures have neuroanatomical and functional connections to the corticostriatal-thalamocortical circuitry. The basal ganglia contain multiple output channels and their dysfunction might result in motor or cognitive dysfunction.38-41 In this context, involuntary movements are identified as a consequence of disruption of the normal control of the basal ganglia. The abnormal pattern of neuronal discharge in the motor circuit could lead to involuntary activation of fragments of movement.42 This would be consistent with the recent findings that primary motor and premotor areas control sets of synergistic muscles rather than a single muscle or just one specific action.43 Tourette's syndrome might be interpreted as an overriding abnormal neural activity of the motor circuit involving multiple outputs from the basal ganglia.
The ZI and VL/LM lesioning has been earlier reported as an alternative approach for controlling involuntary movements.30 44 45The role of intralaminar nuclei (LM) in pathogenesis and in surgery for Tourette's syndrome has been stressed previously.24 46 47 VL/LM surgery alone was performed in one out of 16 patients (patient 7, table 6). Consequently we were not able to compare thalamic targets after infrathalamic lesioning. Additionally, ZI lesioning, as a separate target from the subthalamotomy, has to be delineated. The infrathalamic region, defined as an area between the thalamus and subthalamic nucleus (STN), consists of ZI and the main output and input pathways within pallidal-subthalamothalamic and thalamic-cerebellar circuits. The volume of the ZI is highly variable.48 The primary effect of ZI lesioning could result in alteration of basal ganglia output rather then in ZI lesion itself (fig 3).15 44 46 49This view might be supported by different immediate side effects of pallidotomy, subthalamotomy, and ZI lesioning (table6).34 44 50 51 In our series the reported intraoperative complication of hemiballism was due to STN coagulation. Future lesion position studies might clear the validity of basal ganglia output lesioning as named as infrathalamotomy against subthalamotomy.

{kind=link}
{kind=link}
{kind=link}
Depiction of the zona incerta exact lesion site in the sagittal plane at the coordinates 12 mm behind the ventral border of the foramen of Monro, 3–5 mm under the foramen of Monro and posterior comissure line and 9 mm lateral to the border of the third ventricle. Infrathalamic lesioning might primarily affect the basal ganglia output pathways. VL=nucleus ventrolateralis thalami; LM=lamina medullaris thalamus; STN=subthalamic nucleus; SN=substantia nigra; IC=internal capsule; H1 and H2=fields of Forel.
Four approaches are currently available for neurosurgical treatment of intractable Tourette's syndrome: psychiatric surgery (limbic leucotomy, cingulotomy), ZI and VL/LM lesioning, and a novel combination of cingulotomy and infrathalamic lesioning.12 33 44 52 Recently reported high frequency stimulation (deep brain stimulation) of the right thalamic intralaminar nuclei seemed to reduce the risk of permanent morbidity and inadequate side selection.24 None of the methods has been found to be superior by valid statistical methodology.15 The ZI and VL/LM targets could be chosen for alleviating the involuntary movement component of Tourette's syndrome symptomatology. The psychiatric surgery might improve effectively the overlapping obsessive compulsive behaviour phenomena.12 52-55 Target selection might be based on the most functional disabling symptoms of malignant Tourette's syndrome.
Conclusions
Medically intractable Tourette's syndrome, here defined as malignant Tourette's syndrome, shows progression in tic symptomatology and conversion of waxing and waning phenomena. Our results indicate that unilateral ZI and VL/LM lesioning selected by asymmetry of symptoms provided an effective control of tic severity. The long term motor tic reduction seemed to be less predictable but significant. More than 50% of immediate morbidity after ZI and VL/LM lesioning was transient. In cases of attenuation of contralateral symptoms, surgical intervention on the relevant side could efficiently reduce tic severity but with higher risk of permanent morbidity. The exact target site of infrathalamic lesion needs to be delineated. An adequate selection of the side of first intervention might prevent the patient from increased risk of further surgery. Neuroimaging outcome studies may clarify the exact role for neuroimaging in target and side selection. Deep brain stimulation techniques might lower the risk of inadequate side selection and permanent morbidity. A prospective randomised study including the quality of life domain is needed to validate the role of surgery in the management of malignant Tourette's syndrome.
Acknowledgments
The present work was supported by DAAD grant No A/99/06567. We thank Dr Elias Milios for his collaboration.