Article Text

Abstract
OBJECTIVES Deficits in the maintenance of attention may underlie problems in attention deficit hyperactivity disorder (ADHD). Children with ADHD also show asymmetric attention deficits in traditional lateralisation and visuospatial orienting tasks, suggesting right hemispheric (and left hemispace) attentional disturbance. This study aimed to examine the lateralisation of selective attention in ADHD; specifically, the effect of a moving, random dot background, and stimulant medication in the line bisection task.
METHODS The performance of children with ADHD, on and off methylphenidate, was examined using a computerised horizontal line bisection task with moving and blank backgrounds. Twenty children with a DSM-IV diagnosis of ADHD participated with 20 controls, individually matched for age, sex, grade at school, and IQ. Twelve of the 20 children with ADHD were on stimulant medication at the time of testing. Horizontal lines of varying length were presented in the centre of a computer screen, with either a blank background, or a moving, random dot field. The random dots moved either leftward or rightward across the screen at either 40 mm/s or 80 mm/s.
RESULTS The children with ADHD off medication bisected lines significantly further to the right compared with controls, who showed a small leftward error. Methylphenidate normalised the performance of the children with ADHD for the task with the moving dots.
CONCLUSIONS These results support previous evidence for a right hemispheric hypoarousal theory of attentional dysfunction, and are consistent with the emerging picture of a lateralised dysfunction of frontostriatal circuitry in ADHD.
- attention deficit hyperactivity disorder
- lateralisation
- stimulant medication
Statistics from Altmetric.com
Attention deficit hyperactivity disorder (ADHD) is a complex neurological syndrome of largely unknown aetiology. Genetic factors have been implicated, as have such environmental factors as developmental and birth related brain insults. Its primary symptoms include impulsivity, inattention, and hyperactivity, with additional symptoms including motor restlessness and emotional lability.1 2 For a diagnosis of ADHD, the child must have exhibited some hyperactive, impulsive, or inattentive symptoms before the age of 7 years, although between 30% and 60% of those who have ADHD in childhood continue to exhibit clinical symptoms in adulthood.2
Evidence is accumulating that the problems with inhibiting impulsive actions and difficulty in focusing and sustaining attention may be due to a lateralised disturbance in frontal lobe network function, mediated by the underactivity of predominantly right hemispheric frontostriatal regions.1 3-5 The constellation of symptoms suggest that ADHD is primarily a result of disruption in subcortical-cortical pathways involved in the regulation of behavioural inhibition and efficient executive functioning.6 7 When a stimulant such as methylphenidate is administered, normalisation of arousal levels may occur within structures that are involved in moderating response inhibition and arousal.1
Frontal lobe involvement is supported by clinical findings of executive function deficits such as increased spontaneity, the inability to operate in favour of a remote or abstract reward, a decreased capacity to self monitor behaviour, a decreased ability to respond to stimuli or follow commands, and difficulty maintaining sustained attention.2 8 The caudate has also been implicated in the past with patients with lesions exhibiting typical behavioural patterns of ADHD, including disinhibition, reduced attention span, impulsivity, and socially inappropriate behaviours.9
Neuroimaging research suggests a general hypoarousal dysfunction which may be lateralised to the right basal ganglia-thalamocortical system. Magnetic resonance imaging with a large sample of children with ADHD found that they did not show the normal right>left asymmetry of the caudate nucleus.3 In addition, the asymmetry (left>right) of the lateral ventricle was reversed, and a smaller right globus pallidus, right anterior frontal region, and cerebellum were found in the children with ADHD. In another study,10 no significant asymmetries of the caudate were found for 11 adolescents with ADHD or the control group; however, the ADHD group had a larger right caudate than the controls. In addition, a small sample of six children with ADHD showed a hypoperfused right striatum compared with controls using the SPECT technique, and this hypoperfusion was partially reversible with methylphenidate, which was in accordance with the transient clinical improvements found.4
Voeller and Heilman11 reported that among children with known right hemispheric damage, a large proportion was also diagnosed with ADHD. They therefore performed a letter cancellation task (a typical laterality task) with an ADHD group. Seven right handed children with attention deficit disorder with or without hyperactivity, behaved similarly to adults with right hemispheric damage who typically show neglect of the left hemispace. In the task the children with ADHD made more overall errors of omission than their controls, and there was a significant majority of left sided errors (they detected significantly more targets on the right side of the page than on the left), suggestive of a disturbance in selective or spatial attention. In another study12 a 10 year old boy with no detectable structural brain damage, but several clinical signs of left unilateral neglect and ADHD, showed a significant impairment in sustained attention, as well as lateralised attentional biases (typical of left neglect), such as rightward deviations in a line bisection task and left sided omissions in a letter cancellation task. The attentional deficit in ADHD is seen clinically as the inability to stay on task or focus attention for a prolonged period of time, which is sometimes attributed to an underlying problem of inhibition or self regulation, as are the other core symptoms of ADHD (impulsivity and hyperactivity). Inattentive behaviour also fluctuates according to factors such as motivation levels, environment, and fatigue.13
Although there is no documented evidence of clinical differences for left versus right sides of space, lateralisation studies suggest an asymmetry in controlled attentional orienting in ADHD, implying a right hemispheric dysfunction. Recent research has indicated that people with lateralised attentional problems (for example, unilateral neglect) may also exhibit deficits in sustained attention.14 It is therefore important to ascertain the incidence of lateralised attentional problems in populations that manifest predominantly sustained attention deficits (such as ADHD).
In the present study a computerised horizontal line bisection task (with or without a moving, random dot pattern in the background) was used to examine the lateralisation of selective attention in ADHD. In a previous study of patients with right hemispheric damage with left neglect,15 we found that the moving pattern systematically biased patients’ bisection judgements. We hypothesised that children with ADHD may be unable to ignore such irrelevant background noise due to an underlying deficit in selective attention. Given that children with ADHD have shown an apparent right hemispheric dysfunction in covert orienting and lateralisation tasks, it was predicted that they should show a rightward bias, and be abnormally affected by irrelevant background stimuli, as found for patients with unilateral neglect.15 As a further manipulation, we also examined the effect of stimulant medication on possible anomalies in line bisection performance, by comparing children on stimulant medication with those who had never received stimulants, or who had taken their last dose more than 16 hours previously. It was predicted that the stimulant medication should reduce or normalise any bisection performance differences found for the children with ADHD compared with controls.
Patients and methods
PATIENTS
Participants were 20 children, who were initially referred to the ADHD clinic at Monash Medical Centre with suspected ADHD, or who already had a diagnosis of ADHD and whose parents attended the local ADHD Support Group. All children met the DSM-IV criteria for ADHD.16 Diagnoses of the children who came through the clinic were made by initial clinical interviews with children and parents and follow up cognitive, language, and educational assessments of the child. In addition, all children with ADHD scored >1.5 SD above the mean for age and sex on the ADHD rating scale.17 The ADHD rating scale is a 14 item parent or teacher report checklist developed by R Barkley and G DuPaul for evaluating the occurrence of ADHD symptoms in children (6–12 years of age). Each of the 14 items is based on a particular requirement of the DSM III-R, and normative data from a large sample of normal children has been reported along with reliability and validity data (DuPaul 1990, unpublished manuscript; cited in Barkley, 199018).
The sample of 20 children with ADHD was separated into two groups; 12 were on their normal stimulant medication regimes (methylphenidate) at the time of testing, which was carried out at an average of 2.2 hours after the last dose. The other eight children either had never received stimulant medication, or had taken their last dose at least 16 hours earlier, for the purpose of testing (when any residual drug would probably no longer be affecting behaviour). The mean age of the sample on medication was 10 years, 5 months (range 9 years, 1 month-12 years, 7 months), and the sample off medication was 10 years, 6 months (range 8 years, 9 months-12years, 9 months).
Each child with ADHD was individually matched for age (±9 months), sex, handedness, grade at primary school, and IQ (±10 points) as measured by the Wechsler intelligence scale for children (WISC) or the Kaufman brief intelligence test (KBIT).19 Table 1 gives the demographic details of the ADHD sample on medication and their matched controls, and table 2 the details of those off medication and their matched controls.
Demographic details of the patients with ADHD on medication and matched controls
Demographic details of patients with ADHD off medication and matched controls
All children (children with ADHD and matched controls) were given a cognitive assessment, either on the WISC-III if they came through the ADHD clinic, or the KBIT.
Independent sample t tests indicated that the medicated children with ADHD and controls did not differ with respect to age (t(22)=0.05, p=0.96), grade at primary school (t(22)=0.16, p=0.88), or IQ level (t(22)=0.70, p=0.49); however, the ADHD group had a significantly higher score on the ADHD rating scale than controls (t(22)=15.39, p<0.001). Similarly, the children with ADHD off medication and controls did not differ with respect to age (t(14)=0.97, p=0.35), grade at primary school (t(14)=0.89, p=0.39), or IQ level (t(14)=0.00, p=1.0); however, the ADHD group off medication had a significantly higher score on the ADHD rating scale than controls (t(14)=7.07, p<.001). The ADHD group on medication did not differ from the group off medication for the scores on the ADHD rating scale(t(18)=0.89, p=0.39).
APPARATUS AND PROCEDURE
The line bisection task was presented on a Toshiba 3100SX portable computer with a VGA monochrome screen (active area=148 mm (height)×198 mm (width)). Stimuli (lines, cursor, and dots) appeared amber on a black background. A grey plastic border surrounded the active display, which did not have any marks that could be used by the participants as cues. The task was a horizontal line bisection task with or without moving dots in the background. Participants sat at a table throughout the task, with the display positioned at a distance of around 450 mm and aligned with the midline. A response box (with 2 microswitch buttons 48 mm apart) was located directly in front of the computer keyboard. The participant used the left index finger for the left button, and the right index for the right button. A solid horizontal line (2 mm thick) was presented in the centre of the screen at the beginning of each trial. A vertical cursor (1 mm width×8 mm height) was located at either the left or right end of the horizontal line.
The participants were instructed to move the cursor to the judged centre of the line, and to ignore any moving dots in the background, by pressing buttons to move the cursor leftward (left button) or rightward (right button). The task was self paced, and participants were able to move the cursor to and fro until satisfied. They then pressed another button located in the centre of the front panel of the response box, to record the response and move to the next trial. If, after making their response, the participants were not happy with their previous judgement of the centre, they could repeat the trial. The display remained blank between successive trials. No feedback on accuracy was given. The velocity of the cursor was set at 60 mm/s for all groups. The computer recorded the distance of the cursor from the actual centre of the line to an accuracy better than 1 mm (in the horizontal axis).
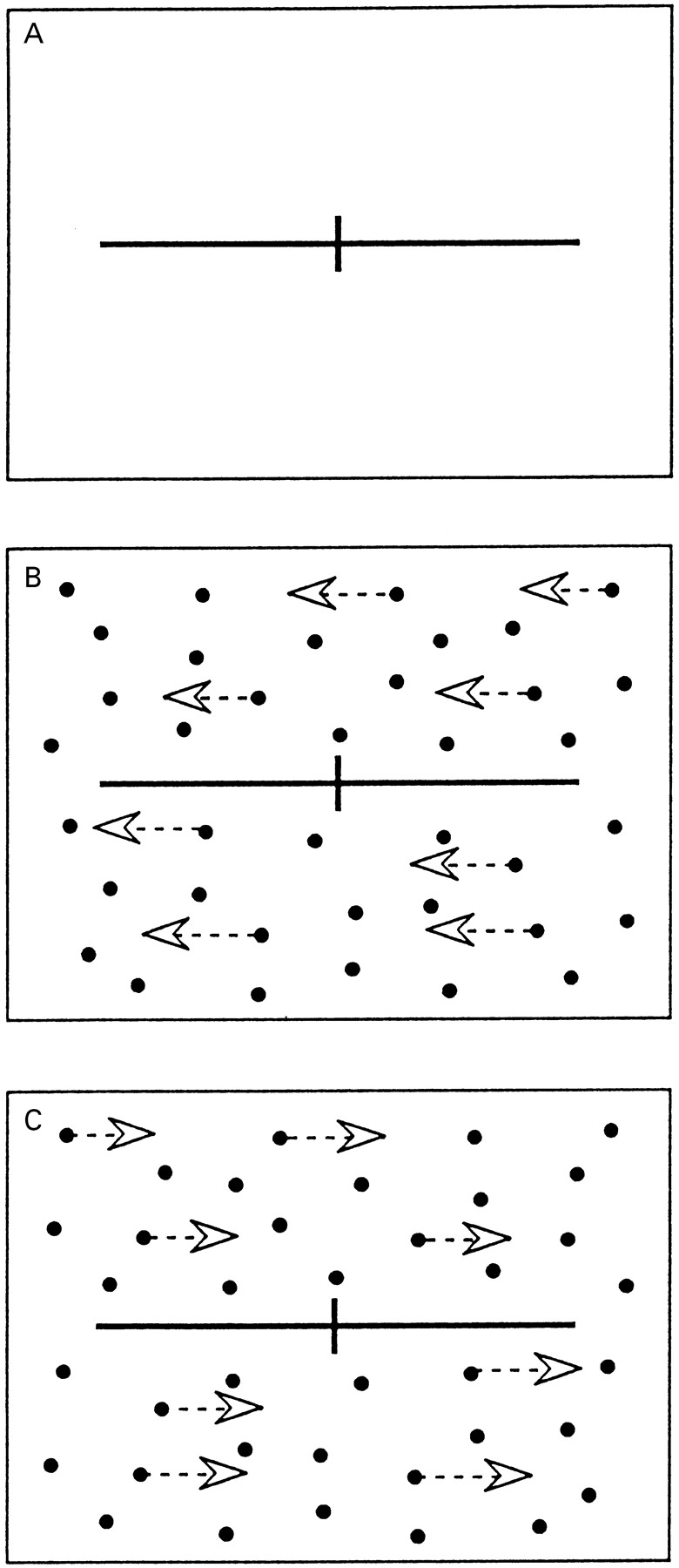
There were five different backgrounds which were pseudorandomly allocated to each of 60 trials. The baseline condition was a blank screen, and there were four different moving dot conditions. The array of solid circular moving dots was displayed in random formation across the active area of the screen at a constant density of 40 dots (20 above and 20 below the line). Two of the four conditions involved leftward drifting dots at either a slow speed of 40 mm/s, or a fast speed of 80 mm/s. In the other two conditions the dots drifted rightward, again at either slow or fast speeds. Therefore, there were 10 conditions, each consisting of six trials. The background dots drifted across the screen and disappeared on one side before re emerging on the other. It is important to note that the dots did not appear within the narrow band that contained the stimulus line and cursor, and thus there was no contiguity between the central display and the peripheral background. Two line lengths were used (180 mm and 140 mm) to minimise the likelihood that participants would develop a single response set and perform the task automatically. Line length and side of cursor start were counterbalanced within the design. Each participant completed a total of 60 trials—that is, 20 trials in each of three blocks—and the order of the blocks was counterbalanced between participants. Figure 1 shows the three different display conditions.

Background screen conditions for the line bisection task: (A) no background (blank screen); (B) leftward moving dots; (C) rightward moving dots.
All procedures followed were in accordance with the ethical standards of the Monash University standing committee on ethics in research on humans, and the Monash Medical Centre human research and ethics committee.
Results
The ADHD group off stimulant medication are considered first. Figure 2 shows the mean deviation from the centre (mm) in the line bisection task for each group and for each screen condition (data were collapsed across the two line lengths for all comparisons). A score of zero indicates bisection at the midpoint, positive values are transections to the right of the centre, and negative values are transections to the left. On average the ADHD group transected the line 1.1 mm to the right, whereas, as normally found,20controls transected the line 1.1 mm to the left.

Mean deviation from centre (mm) for each background screen condition for children with ADHD off medication and controls.
A two way analysis of variance (ANOVA) with factors group (ADHDv controls) and screen (blank screen, slow, and fast dots) showed a main effect of group (F(1,14)=11.17, p<0.01), but no interaction. Thus the ADHD group was significantly right biased compared with the controls, irrespective of the background. One tailed single sample t test (comparing mean bisection errors with zero—that is, perfect bisection) results indicated that the ADHD group was transecting the line significantly to the right of centre (t(7)=2.13, p<0.05), and controls to the left of centre (t(7)=−2.35, p<0.05).
Figure 3 shows that the ADHD group on medication was more accurate than controls when the moving dots were in the background, and that accuracy declined for both groups in the blank screen condition; the ADHD group on medication transected further to the right, whereas controls again transected further to the left. A two way ANOVA with factors group and screen was conducted for the ADHD sample on stimulant medication, and a significant group×screen interaction was found (F(2,44)=3.89, p<0.03). There was not, however, a main effect of group (F(1,22)=2.26, p>0.05).

Mean deviation from centre (mm) for each background screen condition for children with ADHD on medication and controls.
One way ANOVAs comparing the groups for each screen condition showed that the only significant group difference was for the blank screen (F(1,22)=6.94, p<0.02). Thus compared with the controls, the medicated ADHD group transected further to the right for this condition only. One tailed t tests indicated, however, that for this condition, the apparent right transection of the ADHD group was not significantly different from zero (t(11)=1.51, p>0.05). Nevertheless, the control group was again transecting the line significantly to the left of centre (t(11)=−1.85, p<0.05. Thus whereas the unmedicated ADHD group was significantly right biased (and matched controls were left biased), the group on medication showed no significant bias.
POST HOC COMPARISON
To assess whether sustained attention played a part in the asymmetric performance of the ADHD group, two way ANOVAs followed by one tailed single sample t tests were carried out for the first block of 20 trials (block 1) and the final block of 20 trials (block 3) for each of the group comparisons. A two way ANOVA with factors group (ADHD off medicationv controls) and block (block 1v block 3) showed no group×block interaction (F(1,14)=1.42, p>0.05), perhaps due to lack of power (fig 4). Single samplet tests showed, however, that whereas the ADHD group did not deviate significantly from the centre for the first block of trials (t(7)=0.74, p>005) there was a significant right deviation in the third blockt(7)=2.33, p<0.05) The matched controls showed a significant leftward deviation from centre for both the first (t(7)=−2.10, p<0.05), and the third block of trials (t(7)=-2.70, p<0.05).

Mean deviation from centre (mm) for the first and third blocks for children with ADHD off medication and controls.
A further two way ANOVA comparing the larger ADHD group on medication and their matched controls disclosed a significant group×block interaction (F(1,22)=4.56, p<0.03) (fig 5), indicating an increase across blocks in rightward deviation for the ADHD group on medication. However, single samplet tests (comparing mean bisection errors with zero) failed to reach significance for either the first block, (t(11)=−1.10, p>0.05, or the third block of trials (t(11)=1.09, p>0.05). The matched control group showed no significant deviation from the centre for the first block of trials (t(11)=−1.55, p>0.05), but for the third block of trials the left deviation became significant (t(11)=−2.10, p<0.05); this, however, probably reflects reduced variance across blocks as the magnitude of the deviation actually reduced slightly in the third block.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean deviation from centre (mm) for the first and third blocks for children with ADHD on medication and controls.
Discussion
The line bisection task showed that the ADHD group off medication was significantly right biased, compared with the controls’ left bias across all screen conditions. Consistent transections to the right of centre suggest that the left portion of the line was perceived as slightly shorter, or less salient, than the right portion, due perhaps to a reduced ability to direct attention leftward, or perhaps the right portion was perceived as slightly longer. The ADHD group on stimulant medication did not, however, show a significant right bias. Thus, methylphenidate seems to have normalised the ADHD group’s performance, especially with the moving dots in the background. Only when on medication were there no lateral biases in performance; the average point of transection of the ADHD group on medication did not significantly deviate from the true midpoint.
In addition to the traditional lateralisation tasks, children with ADHD have also shown attentional asymmetries in visual-spatial orienting tasks. Carter et al 21 compared 20 unmedicated children with ADHD with their normal controls. Participants maintained central fixation, responding when they detected a target in the left or right visual field. The left or right side of the fixation cross was illuminated before the onset of the target, forming an “arrow cue” which either correctly predicted the target’s location (80% of spatially informative cues were valid) or pointed to the direction opposite to which the target would subsequently appear (20% invalid trials). A neutral cue gave no predictive information (the brightening of the entire fixation cross). The “cost” of an invalid cue was measured as the difference in reaction times for invalidly cued and neutral cued targets. For both groups, the invalid cues were responded to more slowly, as predicted; however, the children with ADHD showed a loss of costs on attentional orienting to invalidly cued left visual field targets. The normal control group, by contrast, showed costs on invalid trials on both sides. These findings suggest a hemispheric asymmetry of “controlled” spatial orienting processes in ADHD.21
In addition to their endogenous spatial orienting task, an exogenous or automatic orienting task indicated the spatial location of the target by a peripheral precue (the brightening of a box either to the left or right of fixation). Invalid cues for left visual field targets (presented to the right of fixation) were significantly more disruptive than invalid cues for right visual field targets.21 This performance asymmetry was not found for the normal controls, but is, however, commonly found for patients with right hemispheric neglect.22 Increased costs of invalid cues for left visual field targets were also evident in a group of adult patients with ADHD in a similar visuospatial attention task.23
In another exogenously cued orienting task,24 children with ADHD failed to show the expected performance asymmetry for invalid precues (the difference occurring in the expected direction but failing to reach significance),21 but did exhibit significantly slower reaction times to the uncued left visual field targets compared with uncued right visual field targets. In addition, low doses of methylphenidate equalised the left and right visual field responses to the uncued targets.
In comparison with the right bias of the unmedicated ADHD group, controls consistently showed a slight but significant left bias. This result is consistent with previous research involving both visual and kinaesthetic line bisection tasks, in which normal right handed people judge the centre of the line to be slightly (but significantly) to the left of the true centre.20 25 26 Neuroimaging and cognitive studies of normal people, as well as animal studies, suggest the involvement of right hemispheric cortical regions (in particular the right prefrontal cortex) in selective attention and arousal and vigilance.27 Alertness (a general readiness to respond, or vigilance) and selective attention (selectively or spatially focused attention with concomitant inhibition of distracting stimuli) may be considered as two component functions of a general attention mechanism.28 Right hemispheric lesions may impair sustained alertness29-31 and selective/spatial attention32-34 in humans. There is also increasing evidence that mechanisms subserving spatial attention and alertness are related; thus patients with right hemispheric unilateral neglect show a bilateral deficit in sustained attention in addition to the well documented spatial attentional deficit on the contralesional side of space.35 Moreover, the lateralisation of attentional dysfunction in neglect is linked to low arousal levels.28
Line bisection performance in the present study can be contrasted with that of left neglecting patients with right hemispheric damage, who were previously shown to bisect lines to the right in the same paradigm.15 The performance of patients with neglect, however, was also affected by the direction of background movement, such that the patients’ judgements were significantly shifted toward the “neglected” or left side by the leftward moving background.15 The children with ADHD in the same task showed the expected, but relatively small, right sided bias in line bisection; however, the leftward moving dots did not shift the bisection judgements to the left. In fact, unlike the situation with right hemispheric damage, the direction of the moving dots did not affect the performance of the children with ADHD at all. Thus whereas children with ADHD may perform similarly to patients with unilateral left neglect in some traditional lateralisation tasks (for example, letter cancellation and line bisection),11 there are seemingly both quantitative and qualitative differences in the task performances of these groups. Firstly, the magnitude of the error in tasks such as line bisection were comparatively small for the ADHD group. The average error for the unmedicated children with ADHD in this task was about 1 mm to the right of centre, compared with the typically variable, but substantially larger, bisection error for patients with left neglect.36-38 Although the ADHD group does not seem to have the same “stickiness”22 of attention as the patients with neglect (as their lateralised performance is independent of the moving background), the lack of an effect of background movement could be an artefact of the small bisection error for the ADHD group. Further investigation is needed to elucidate the effect of background motion on lateralised task performance in ADHD.
Sustained attention may have also played a part in the bisection performance of the children with ADHD. The children with ADHD off medication showed a significant temporal sequence effect. Their bisection performance did not deviate from the centre in the first block of 20 trials, but in the third block of trials their right bias emerged. The children with ADHD on medication showed no significant deviation from the centre for the first or third block of trials. Thus (for the children with ADHD off medication) as the task became more familiar, arousal levels and sustained attention most probably decreased. Evidence for a coupling of low levels of alertness and the presence of lateralised biases was provided in a recent study in which patients with right hemispheric damage (with unilateral left neglect) showed the expected problems in attending to visual stimuli on the left; however, an uninformative sound (presented immediately before presentation of the visual target) “alerted” the patients and reduced the lateral bias in spatial attention.28 The sustained attention deficit in ADHD is likely to have resulted in a decreased alertness over time for the line bisection task, and thus caused emergence of a right bias in the final block of trials. The children with ADHD on stimulant medication, however, did not show the same abnormal bias, due probably to an improved level of arousal.
The well documented sustained attention deficits in ADHD are thought to be due to low levels of neural activation in prefrontal structures, accompanied by an imbalance of activity in frontostriatal regions.39 The deficit in the frontostriatal gating mechanism not only results in a sustained attention deficit, but is also thought to be responsible for the impulsivity and hyperactivity.6 39 Conceivably, the three core features of ADHD (including a deficit in sustained attention) may be explained by this dysfunctional gating mechanism, and the disinhibition of responses to sensory information.39 The underlying mechanism of the lateralised spatialattention deficit in ADHD is conceivably the higher level of left hemispheric activation (right hemispherichypoarousal, consistent with the reversal of normal asymmetry of basal ganglia structures3 4) that results in the slight rightward shift of attention. However, the clinical manifestation of this small, yet significant, bias in spatial attention would be negligible.
In conclusion, this study found children with ADHD to be abnormally right biased in line bisection. Methylphenidate medication normalised this asymmetry, perhaps by increasing an underlying (right hemispheric) hypoarousal. The present findings support an account of right hemispheric hypoarousal in ADHD,11 resulting in a deficit in both arousal and left side selective attention. Neuroimaging studies further support such a hypothesis.3 4 More research should now focus on the spatial (as opposed to the sustained) aspect of attention deficit in ADHD.
Acknowledgments
This research was supported by the Australian Research Council.