Article Text

Abstract
Between 10 and 30% of patients seen by neurologists have symptoms for which there is no current pathophysiological explanation. The objective of this review is to answer questions many neurologists have about disorders characterised by unexplained symptoms (functional disorders) by conducting a multidisciplinary review based on published reports and clinical experience. Current concepts explain functional symptoms as resulting from auto-suggestion, innate coping styles, disorders of volition or attention. Predisposing, precipitating, and perpetuating aetiological factors can be identified and contribute to a therapeutic formulation. The sympathetic communication of the diagnosis by the neurologist is important and all patients should be screened for psychiatric or psychological symptoms because up to two thirds have symptomatic psychiatric comorbidity. Treatment programmes are likely to be most successful if there is close collaboration between neurologists, (liaison) psychiatrists, psychologists, and general practitioners. Long term, symptoms persist in over 50% of patients and many patients remain dependent on financial help from the government. Neurologists can acquire the skills needed to engage patients in psychological treatment but would benefit from closer working relationships with liaison psychiatry or psychology.
- DSM-IV, Diagnostic and Statistical Manual of Mental Disorder, 4th edition
- ICD-10, International Statistical Classification of Diseases, 10th revision
- dissociative disorder
- functional symptoms
- neurology
- psychotherapy
- somatoform disorder
Statistics from Altmetric.com
- DSM-IV, Diagnostic and Statistical Manual of Mental Disorder, 4th edition
- ICD-10, International Statistical Classification of Diseases, 10th revision
In a typical neurology outpatient clinic, 10–30% of patients will have symptoms which are not explicable by demonstrable structural or pathophysiological abnormalities.1 Unexplained symptoms are particularly common amongst frequent users of healthcare services.2 Up to two thirds of these patients have symptomatic psychiatric comorbidity and many describe suicidal ideation if asked.3,4 Neurologists need to be able not only to diagnose symptoms as functional but also to communicate with and manage patients in whom no clear organic explanation for symptoms can be found. This article addresses some of the common questions which neurologists face when they see patients with functional symptoms.
WHAT ARE FUNCTIONAL SYMPTOMS?
Functional symptoms are physical complaints postulated to be associated with psychological distress, which are not primarily explained by pathophysiological or structural abnormalities. This explanation sounds succinct but suffers from several conceptual limitations. Firstly, the diagnosis depends on the exclusion of a medical explanation by clinical judgement or investigation (which may be impossible in paroxysmal disorders like epilepsy, or in conditions like migraine, in which the diagnosis relies on the subjective assessment of the examiner). Secondly, psychological distress is difficult to measure or objectify. Thirdly, functional symptoms can complicate medically explained disease processes which can cause difficulties with delineation and diagnosis.
Functional symptoms can mimic those of most recognised neurological disorders (fig 1), manifest acutely or as a more indolent problem, and can be persistent or intermittent in nature. Functional symptoms can occur together with symptoms of neurologically explained disorders or may be the defining manifestation of a functional disorder.

Distribution of 717 functional symptoms in 405 neurology patients.19
WHAT NAME SHOULD WE USE FOR FUNCTIONAL SYMPTOMS?
Functional symptoms have attracted many different terminologies. Some diagnostic labels which were initially acceptable had to be abandoned because they entered common usage as derogatory idioms.5 Appropriate terminology is important because the explanation of functional symptoms is an important part of treatment, and the acceptance of the explanation given is associated with a better prognosis.6,7 This communication may be hindered if patients feel that their symptoms are interpreted by the doctor as malingering or exaggeration. A recent study has demonstrated that “functional” is more acceptable to patients than the terms “psychosomatic”, “medically unexplained”, or “stress related”.8 In case of seizures, “functional” proved less offensive than “hysterical”, “pseudo”, “stress related”, and “psychogenic” or the expression “non-epileptic attack disorder”.9 The term functional also lends itself to offering patients a positive explanation of symptoms (for example, “there is no damage of nerve cells but a disruption of function”).
In the current taxonomies (Diagnostic and Statistical Manual of Mental Disorder, 4th edition (DSM-IV),10 International Statistical Classification of Diseases, 10th revision (ICD-10)11) functional symptoms can be classified as manifestations of somatoform disorders (physical symptoms which suggest a general medical condition) or dissociative disorders (disruption of the usually integrated functions of consciousness, memory, identity, or perception). However, many functional neurological symptoms (like amnesia or seizures) fulfil diagnostic criteria for both categories. Perhaps because of this, the present clinical criteria in the ICD and DSM systems do not perform well diagnostically if relied upon alone.12 What is more, the term “somatoform” does not imply a positive explanation for the symptom, and there have been increasing criticisms of the somatoform classification with more emphasis being placed on symptomatology.13
Functional symptoms were previously called “hysterical”, but the term’s derogatory connotations and the ever widening meaning of the word (for example, mass hysteria, hysterical personality) make it inappropriate.5 Functional problems are sometimes called “psychogenic” or attributed to “conversion”. However, in the ICD-10 the term “psychogenic” is defined quite narrowly as signifying an association with recent trauma,11 and the term “conversion” evokes an aetiological mechanism for which we have no evidence. These models are too simplistic in most cases.
The term “medically unexplained” is a better representation of scientific knowledge to date, but may make patients think that their symptom is not being taken seriously, is unlikely to inspire confidence, and may jeopardise engagement with future therapeutic endeavours.
ARE FUNCTIONAL SYMPTOMS WILFULLY PRODUCED?
In line with the current classificatory systems of mental disorders (DSM-IV, ICD-10), most clinicians attempt to distinguish between functional symptoms (which are not intentionally produced by the patient) from symptoms that are feigned. However, whereas variability of effort can be quantified, intentionality cannot.14 Besides, there may not be a categorical distinction between patients who feign their symptoms and patients who do not.15 Because of this, it is actually not possible to say whether or how often functional symptoms are wilfully produced. Fortunately, it is rarely necessary for a clinician to determine whether symptoms are intentional. Even if patients see no other way of reducing psychological distress than feigning illness or exaggerating pathophysiologically explained symptoms, it may be appropriate to offer medical or psychological attention.16
ARE THERE CLEAR DISTINCTIONS BETWEEN FUNCTIONAL, FEIGNED, AND HYPOCHONDRIACAL SYMPTOMS?
The DSM-IV and the ICD-10 encourage clinicians to divide intentional symptoms into malingered symptoms (wilfully produced for external gain) or factitious symptoms (wilfully produced for internal gain). However, it is very difficult for a clinical observer to judge the internal or external reward for a symptom. Similar problems arise with the concept of “secondary gain” (for example, benefits associated with taking on a sick role).17
The DSM-IV and ICD-10 further distinguish between somatoform disorders (which are characterised by functional symptoms) and hypochondriasis, in which there is predominant anxiety about illness, often in the presence of misinterpretation of physiological processes in the body. However, somatoform disorders are often also associated with anxiety about “serious” underlying pathology, and this categorical distinction may be difficult to make.
This does not mean that there is no difference between patients whose functional symptoms are unintentional, malingered, factitious, or hypochondriacal. The margins between these conditions are simply not as clear as the prototypical definitions in the DSM-IV and ICD-10 suggest.
ARE FUNCTIONAL SYMPTOMS DISPROPORTIONATELY PREVALENT IN NEUROLOGY?
Although many who have written about functional symptoms (Thomas Willis, Jean-Martin Charcot, Joseph Babinski, Sigmund Freud, to name but a few) had a neurological background, a comparative study found that functional symptoms were similarly prevalent in other medical specialties.18 Within neurology, one study found that 9% of 4470 inpatient episodes were provoked by psychogenic disorders,19 and a second reported that 11% of 300 consecutive neurological outpatient presentations were “not at all explained” by organic disease, 19% “somewhat explained”, 27% “largely explained”, and 43% “completely explained”.1 Several reports suggest that the risk of functional symptoms is increased in patients with physical disorders of the brain, or indeed the peripheral nervous system,20–22 but (perhaps because of the indistinct conceptual boundaries) the prevalence of functional symptoms in the context of structural or pathophysiologically explained neurological disorders is unknown.
WHAT CAUSES FUNCTIONAL SYMPTOMS?
Recent attempts to explain functional symptoms have focussed on volition,23 attention,24 and auto-suggestion.25 One attractive model suggests that somatisation represents an innate coping mechanism learned from early parent-child interactions.26,27 The neurobiological substrate of functional symptoms remains elusive, but it is now clear that the brain can physically adapt to environmental challenges and stress,28,29 so scientific understanding has moved beyond the dualistic concept of separation between mind and brain. Functional or voxel based neuroimaging techniques may bridge the gap between theoretical concepts and biological understanding in the future. However, whilst the studies completed to date are promising, they have been small and their results are difficult to interpret.30–33
In the absence of a clear pathophysiological understanding, patients with functional neurological symptoms are perhaps best understood using a multidimensional aetiological model, in line with that proposed for other unexplained somatic disorders.34 This approach can accommodate biographical factors (like childhood trauma, abuse, life events), relevant biological features (like gender), psychological features (like poor coping styles, the tendency to dissociate, emotional expressiveness), neurological co-morbidity (for example learning disability or epilepsy), social aspects (such as a disturbed family environment, financial insecurity, absence of friends or confidants, limited coping resources), and broader cultural factors (such as attitudes to illness, gender roles). The biopsychosocial model of disease developed in the 1980s, which considers the interplay between all these factors, is a helpful conceptual approach in this context.35
The analysis of an individual patient can be informed by a pragmatic distinction between predisposing factors (conferring an increased vulnerability to functional symptoms), precipitating factors (triggering symptoms), and perpetuating factors (contributing to a chronically recurrent course).36 These factors interact with other psychiatric disorders (like anxiety disorders, posttraumatic stress disorder, depression) and personality traits (especially those typical of borderline and dependent personality disorders).37 The importance of the various factors differs substantially between patients and may even change in the same patient over time. In assessing the importance of possible aetiological factors it is important to note that the presence of one particular factor (for instance childhood abuse) does not automatically make it aetiologically relevant.
In many patients a history of trauma, a stressful life event, or an “unspeakable dilemma” can be identified.38,39 Often functional disorders seem to be sparked off by a relatively small event which appears to serve as a symbolic reminder of more serious trauma or distress in the past.40 Even if the identified problem does not seem serious enough to trigger a disabling functional symptom, it may be useful in engaging patients in psychological treatment.
HOW CAN WE DIAGNOSE FUNCTIONAL SYMPTOMS?
The first step in the diagnosis of functional symptoms is the exclusion of a neurologically explained problem. Clinicians have to strike a balance between the pursuit of diagnostic certainty and the fact that continuing investigations may not allow patients to address psychosocial issues and have the potential to cause anxiety and iatrogenic damage. The second, equally important step is the screen for aetiologically relevant psychological or psychiatric features. These are likely to be serious recent life events, but triggers could be more subtle in patients with pre-existing inadequate coping skills. This stress-diathesis model means that explicit psychological criteria for the diagnosis of functional disorder remain elusive although some recent progress has been made.41
The clinical signs of functional weakness and sensory disturbance,42 disorders of gait or stance,42–44 and non-epileptic seizures45,46 have been described in detail elsewhere (table 1).
Of course, the clinical tests or investigations which are required to exclude neurological disorders differ between one symptom and another. Before asking for tests clinicians should attempt to review their patient’s previous health records to avoid needless replication. What is more, thick notes with presentations to many different specialities can also act as a diagnostic pointer.47 When requesting investigations clinicians should consider that tests with a low pretest probability of detecting pathology are associated with a high risk of false positive results. Many tests rely on the detection of inconsistency of the clinical problem (apparent in collapsing weakness or the inability to lift a leg off an examination couch whilst being able to walk). Inconsistency also becomes apparent when the quantitatively poor performance of patients with functional disorders in neuropsychological tests is analysed in a qualitative manner.48,49 In patients with apparent weakness or sensory loss, inconsistency can also be found by demonstrating intact sensory pathways using neurophysiological methods like evoked potentials.50,51
Of course, the detection of inconsistency simply raises the possibility that a conventional syndrome does not fit—it does not follow that a functional disorder must be present. Patients with many neurologically explained disorders show marked diurnal variation or variable symptoms.
HOW CERTAIN CAN WE BE THAT A SYMPTOM IS FUNCTIONAL?
Several recent studies have shown that patients whose symptoms are considered neurologically unexplained after appropriate assessment rarely turn out to be diagnosed with a somatic neurological disorder later. However, it should be born in mind that these studies were carried out at specialist centres, and that the risk of a misdiagnosis of disorders characterised by functional symptoms may be higher in less well investigated patients. Stone et al found that a neurological explanation had been found in one of 42 patients with functional weakness or sensory loss after a mean of 12.5 years of follow up.52 Crimlisk et al found that only three of 64 patients with functional weakness had developed an identifiable somatic disorder explaining the weakness 6 years after the initial assessment (two out of these three patients were misdiagnosed because they had disorders with variable symptoms).5,53 Couprie et al found an unexpected somatic explanation in four of 56 patients with a functional neurological problem after 1.5–9.5 years.54
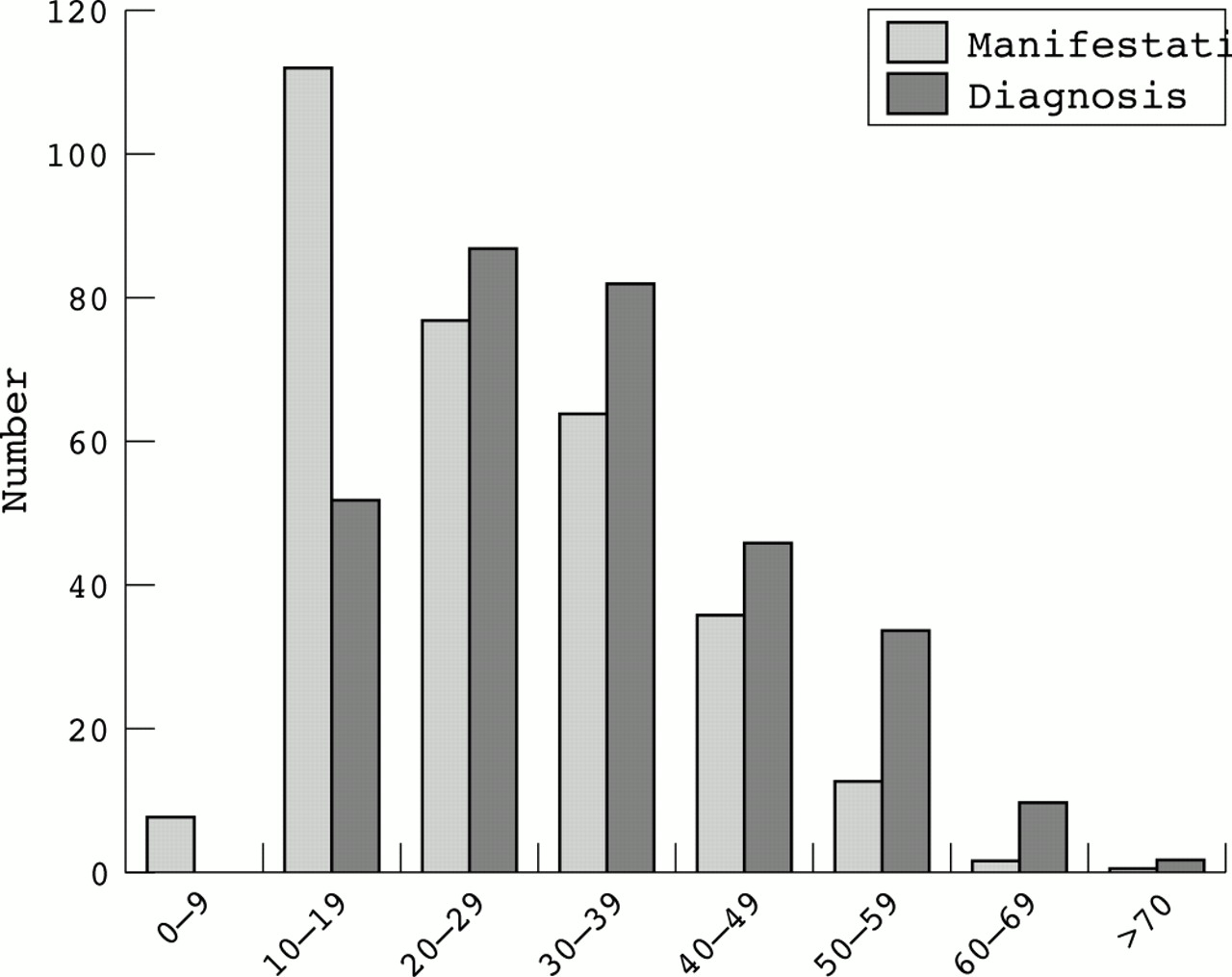
Although it therefore seems that the finding that a symptom is functional usually stands the test of time, physicians have a tendency to underdiagnose functional problems.55 This is likely to be one of the reasons why patients with non-epileptic seizures for instance are often misdiagnosed as having epilepsy for many years56 (fig 2). Several studies have shown that the delay in the diagnosis of functional symptoms is associated with poorer outcome.53,57,58 Patients do therefore not benefit from a delayed diagnosis but may suffer as a result of it. The misdiagnosis of non-epileptic seizures as epilepsy is particularly dangerous—severe iatrogenic injury, pregnancy loss, and death have been reported.59–61 Physicians who fail to identify medically unexplained disorders may be faced with litigation.62
{kind=link}
{kind=link}
Age at seizure manifestation and correct diagnosis of 313 patients with non-epileptic seizures. Almost all patients were thought to have epilepsy and 75.5% had been treated with anticonvulsant drugs.56
This does not mean that neurologists should rush into calling a symptom functional. There are also risks of overdiagnosing functional problems.63,64 In particular, patients with atypical or rare organic disease presentations may not receive appropriate treatment or be denied financial help for incapacity from the government.65 Once a clinician has diagnosed a problem as functional, patients are less likely to be taken seriously by colleagues or to receive palliative or curative treatment.66
In the absence of a diagnostic gold standard, a degree of doubt about a neurologically explained disorder may remain. However, clinicians can usually be sure enough of the functional nature of a symptom to stimulate a search for possible (psychosocial) triggers and associated psychopathology, and to propose psychological forms of treatment.
WHAT IS THE BEST WAY OF COMMUNICATING THE DIAGNOSIS OF A FUNCTIONAL PROBLEM?
The basic communication skills required for patients with functional symptoms do not differ from those which are helpful with other patients.67,68 If the initial communication goes well, symptoms settle in a substantial group of patients.6,69,70 Communication is more likely to be successful if positive diagnostic factors (significant life events, psychiatric features) and negative factors (inconsistencies, negative investigations) have been elicited so that the relevance of psychological factors becomes more believable to the patient.71 A good way to begin is to enquire what the patient’s particular concerns about his symptom are, and what he may have been told by other doctors, so that specific reassurance can be given.
The initial explanation should cover the items listed in table 2. The aims of this conversation include reducing anxiety, instilling a degree of therapeutic optimism, and facilitating engagement in further psychological therapy. Outcome is likely to be better if a positive diagnosis is made (for example, “you have (a) functional weakness/numbness/seizures”), and this diagnosis is explained as much as this is possible (for example, “we are not entirely sure what causes functional weakness/numbness/seizures, but we often see them in patients who are under a lot of stress/who have suffered a loss/who have been badly upset by something…”).72 The physician may pause at this point of the explanation to give the patient a chance to volunteer a relevant traumatic event, conflict, or problem. At no point should the patient be made to feel coerced into making a disclosure, and it should be made clear that the patient should do this only at a time and place with which they feel comfortable. Patients may be probed gently (“I wonder if you recognise any of this in your own life?”).
Management of patients with functional neurological symptoms
The possible co-occurrence of physical and psychological symptoms should be discussed if applicable (stressing that any separation is quite artificial). It may be helpful to include an educational element at this point to help the patient to understand how emotional factors could be causing physical symptoms. This is best given as a three stage explanation, linking mood, pathogenesis, and symptoms (for example, “When people are anxious the muscles in their neck tend to tense up and that can cause headaches”).73
Finally, the neurologist should explain the plan for further management. If symptoms are acute, patients may improve with an explanation, encouragement, positive suggestion, and physiotherapy. In more chronic cases, and to anticipate and prevent relapse, a psychological approach should be considered and offered in most cases.
Neurologists will need to make themselves aware of local pathways of referral for psychological treatment. Ideally this should be closely integrated into the neurological diagnostic and therapy service. Finding a suitable therapist may not be easy because there is little evidence that the provision of psychotherapy services in the National Health Service has improved much since it was last investigated in 1996.74
The practice of copying medical correspondence to patients (which has been endorsed by recent government policy in the UK) offers a further opportunity to enforce the points which were made during the consultation. The effects of this practice have not been studied in the context of functional symptoms, but they have been studied in psychiatric practice.75 Results show that there are many reasons why openness could be particularly helpful in this context. Of course, copied letters will cause offence and confusion if they do not reflect the discussion during the consultation.
SHOULD PATIENTS WITH FUNCTIONAL SYMPTOMS BE REFERRED TO A PSYCHIATRIST?
Many neurologists are uncomfortable continuing to see patients with functional symptoms. As a consequence, they may get little opportunity to improve their clinical practice in this area. Adult psychiatric services have had to focus on so called severe mental illness (that is, bipolar disorder and schizophrenia), and psychiatrists may therefore also have limited expertise in dealing with these problems. The fact physicians seem unable to address their problem is one of the reasons why many patients with unexplained symptoms keep seeking medical advice.2
Ideally, patients with a functional neurological symptoms should be screened for anxiety and depression and should be offered a psychological and psychiatric assessment. Whilst functional disorders do not sit easily within a categorical diagnostic system (see above), there is general agreement that they are a important marker of psychiatric morbidity.76 In one study of 300 consecutive new patients seen in a neurological outpatient clinic, 67% of patients with unexplained symptoms but only 38% of patients with explained symptoms had depressive or anxiety disorders.3 In another study, 33% of patients with functional motor symptoms but only 10% of patients in the control group had a major psychiatric disorder.77 Whereas 13% of patients with unexplained symptoms had seriously considered suicide in the last 2 weeks, only 7% of patients with explained symptoms had done so.4 These results fit with the observations in other areas of medicine that patients with unexplained symptoms are roughly twice as likely to suffer from psychiatric disorders.78 Patients with more unexplained symptoms are at greater risk.79,80
Ideally the psychiatric assessment should be carried out by a psychiatrist with an interest in this area (or by a neurologist with relevant psychiatric skills). Unfortunately, liaison psychiatry services (and neurological services for patients with functional disorders) remain patchy and a substantial group of patients will decline the option of seeing a psychiatrist.3 To some patients, a psychologist may be a more acceptable option (especially if they are part of the neurological team). Good communication between different disciplines is essential to avoid patients being given mixed or confusing messages.
WHAT SPECIALIST TREATMENT IS AVAILABLE?
There are insufficient randomised controlled trials in the area of functional neurological symptoms. Evidence from the treatment of other medically unexplained symptoms and similar disorders, however, supports the hypothesis that psychotherapeutic methods may be helpful in some patients.81–86 The evidence is perhaps strongest for variants of cognitive behavioural therapy.87–89 Psychodynamic, interpersonal therapy, and hypnosis have been shown to be effective treatments for irritable bowel syndrome,90–92 a disorder often comorbid with functional neurological symptoms.93 Furthermore, biofeedback methods may be useful in the treatment of somatoform disorders.94
Little is known about which patients benefit most from which approach. Predisposing and precipitating factors are important in building up an understanding of the patient. However, the mere disclosure of traumatic factors alone is usually not sufficient.95 Therapy needs to focus especially on factors perpetuating symptoms if it is to be of lasting benefit.96 It is important to note that the kind of psychotherapy required is not the same as counselling (schooled listening) which is only likely to help in milder (or self limiting) psychiatric disorders.97
Antidepressants may be useful in the treatment of patients with functional symptoms. They may even be effective for those without a depressive syndrome.98 Antidepressants have been shown to reduce emotional dysregulation,99 a personality trait associated with functional symptoms.100 One of the most common reasons for non-response to antidepressants is an inadequate dose given for an inadequate length of time.101 Neurologists should anticipate that nearly three quarters of neurological outpatients think antidepressants are addictive, and nearly half think they can do physical harm.102 Patients who can see the reasons for taking medication are more likely to complete the course.
Antipsychotic drugs may have a very limited role in the treatment of patients with quasi-psychotic dissociative symptoms resistant to other methods but should be used with caution because of long term side effects.103
DO NEUROLOGISTS NEED TO FOLLOW UP ALL THEIR PATIENTS WITH FUNCTIONAL SYMPTOMS?
Rapid discharge from a neurological clinic may be interpreted by the patient as a sign that the neurologist disbelieves him or her. They may then be forced to rely on financial help from the government, or are left dependent on their family or social support network (we know that patients with non-epileptic attacks are more likely to receive financial help from the government than comparable patients with epileptic seizures104,105). It is often wise to oversee any transfer of clinical care to psychological or psychiatric services as many patients do not engage easily.
Follow up should satisfy a number of aims: (1) to signal to the patient that his complaint is being taken seriously without the need for a further health crisis; (2) to facilitate engagement in a psychological treatment programme; (3) to reduce the risk of referral for a more palatable specialist opinion; (4) to offer the opportunity to review the diagnosis and ensure no alternative pathology has been missed (especially if new symptoms evolve); and (5) to avoid inappropriate diagnostic re-assignment to an organic disorder.
In practice, only a small number of patients with mixed physical and psychological disorders (for instance epilepsy and non-epileptic seizures) will require long term follow up by a neurologist. For patients with chronic medically unexplained symptoms who fail to improve with a psychological treatment programme the focus may shift to the maintenance of social functioning and minimisation of iatrogenic damage. Programmes for the effective management of such patients in primary care emphasise the regular assessment of patients by a single, identified health practitioner to pre-empt crisis generation, the withdrawal of unnecessary medication and specialist referrals, and the setting of achievable goals (damage limitation rather than cure).106 As a minimum these programmes can reduce healthcare usage and cost.107 Some patients may also be open to a process of reattribution. One influential approach to reattribution is based on the three stage process of making the patient feel understood, changing the agenda from a focus on symptoms to a wider view of abilities, and relating symptoms to psychosocial problems.73,108
WHAT IS THE PROGNOSIS OF FUNCTIONAL NEUROLOGICAL SYMPTOMS?
Studies of patients with functional paresis or sensory disturbance show that 37–83% of patients (mean age 36–39 years) continued to have symptoms 2–16 years after diagnosis.52–54,58,109 The study with the longest follow up showed that 29% of patients had retired on medical grounds.52 Outcome was similarly poor in unselected neurological outpatients with medically unexplained symptoms. Symptoms were worse or persisted in 54% of patients 8 months after the original assessment.110 The prognosis appears even worse in patients with non-epileptic seizures. The largest study showed that 71% of patients continued to have seizures 11 years after manifestation, and 56% of patients were dependent on social security.111 Patients who remain unimproved continue to consume healthcare resources. One follow up study of 64 patients with motor conversion symptoms diagnosed at a tertiary neurology referral centre found that 6 years after diagnosis 51% of patients had been re-referred to another neurologist (28% with the same symptom).112
There is a danger that new clinicians unfamiliar with a case will relaunch unnecessary investigations or diagnose organic disease which has previously been ruled out. The investigation of the outcome of patients with non-epileptic seizures found that despite advice to discontinue them, 41% of patients were still taking anticonvulsants 5 years later.111
Even with psychological treatment, outcome is not good in all patients. A long history of physical symptoms, particularly debilitating symptoms and entrenched support systems which reinforce illness behaviour, predict a poor prognosis. The prognosis is better if patients acknowledge emotional distress in relation to their symptoms and in patients with adequate support who live in a stable social environment. Poor compliance or an unwillingness to engage are likely to result in poor outcome.85
CONCLUSION
Functional neurological symptoms are common but poorly understood and frequently mismanaged. After appropriate investigations, clinicians should not be afraid of calling symptoms functional. However, there is a risk of both under and over diagnosis. When neurologists do not follow up such patients themselves diagnostic errors may be perpetuated. The outcome of disorders characterised by functional neurological symptoms is currently poor. Outcomes are likely to improve if the diagnosis of such disorders was sought more actively and communicated more successfully. Whilst many questions about nosology, aetiology, and long term effectiveness of treatment remain open, it is not appropriate to refuse treatment to patients with the biological potential to make a full recovery. Neurologists are well placed to work in collaboration with (liason) psychiatrists, psychologists, and general practitioners to develop treatment programmes for patients with functional neurological symptoms.
REFERENCES
Footnotes
-
Competing interests: none declared